

Effects of adiposity on plasma lipid response to reductions in dietary saturated fatty acids and cholesterol
- PMID: 22332058
- PMCID: PMC3090171
- DOI: 10.3945/an.111.000422
Effects of adiposity on plasma lipid response to reductions in dietary saturated fatty acids and cholesterol
Abstract
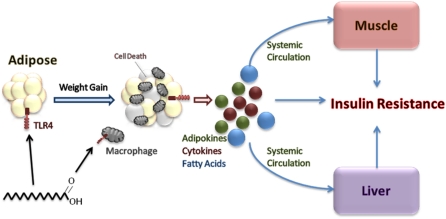
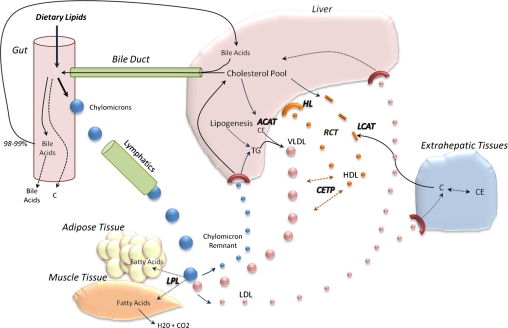
Dietary SFA and cholesterol are major targets for reducing plasma total and LDL cholesterol as a strategy to decrease cardiovascular disease risk. However, many studies show that excess adiposity attenuates the expected lipid and lipoprotein response to a plasma cholesterol-lowering diet. Diets low in SFA and cholesterol are less effective in improving the lipid profile in obese individuals and in patients with metabolic syndrome. In contrast, lean persons are more responsive to reductions in dietary SFA and cholesterol. Multiple mechanisms likely contribute to the altered plasma lipid responses to dietary changes in individuals with excess adiposity. The greater rate of hepatic cholesterol synthesis in obese individuals suppresses the expression of hepatic LDL receptors (LDLR), thereby reducing hepatic LDL uptake. Insulin resistance develops as a result of adipose-tissue induced inflammation, causing significant changes in enzymes necessary for normal lipid metabolism. In addition, the LDLR-mediated uptake in obesity is attenuated by alterations in neuroendocrine regulation of hormonal secretions (e.g. growth hormone, thyroid hormone, and cortisol) as well as the unique gut microbiota, the latter of which appears to affect lipid absorption. Reducing adipose tissue mass, especially from the abdominal region, is an effective strategy to improve the lipid response to dietary interventions by reducing inflammation, enhancing insulin sensitivity, and improving LDLR binding. Thus, normalizing adipose tissue mass is an important goal for maximizing the diet response to a plasma cholesterol-lowering diet.
Conflict of interest statement
Author disclosures: M. R. Flock, M. H. Green, and P. M. Kris-Etherton, no conflicts of interest.
Figures
References
-
- Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112:2735–52 - PubMed
-
- Garrison RJ, Wilson PW, Castelli WP, Feinleib M, Kannel WB, McNamara PM. Obesity and lipoprotein cholesterol in the Framingham offspring study. Metabolism. 1980;29:1053–60 - PubMed
-
- Keys A, Aravanis C, Blackburn H, Van Buchem FS, Buzina R, Djordjevic BS, Fidanza F, Karvonen MJ, Menotti A, et al. Coronary heart disease: overweight and obesity as risk factors. Ann Intern Med. 1972;77:15–27 - PubMed
-
- Grundy SM. Metabolic syndrome pandemic. Arterioscler Thromb Vasc Biol. 2008;28:629–36 - PubMed
