

Functional pace-mapping responses for identification of targets for catheter ablation of scar-mediated ventricular tachycardia
- PMID: 22333344
- PMCID: PMC4334590
- DOI: 10.1161/CIRCEP.111.967976
Functional pace-mapping responses for identification of targets for catheter ablation of scar-mediated ventricular tachycardia
Abstract
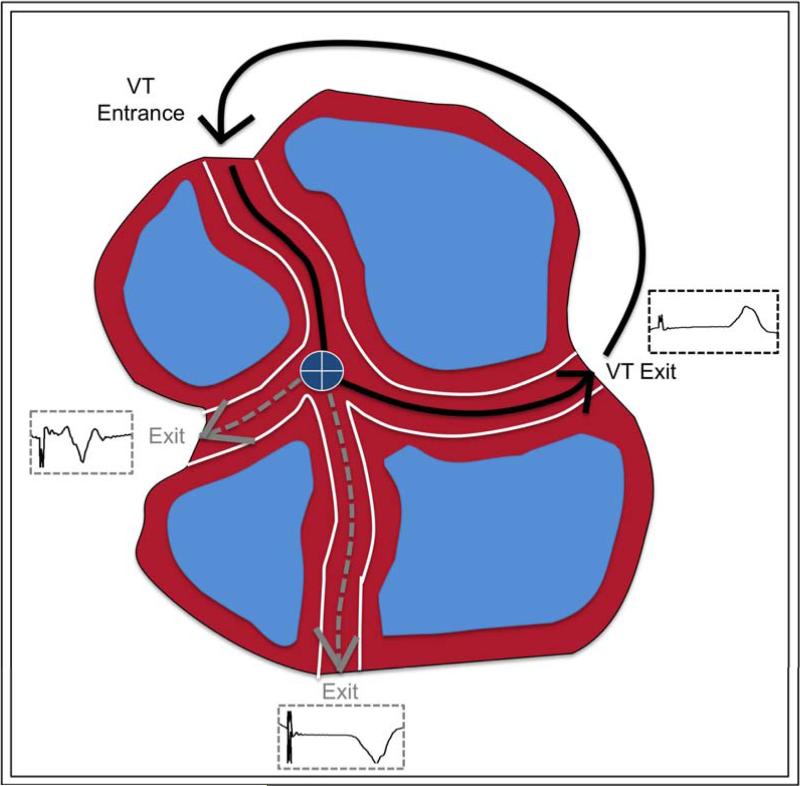
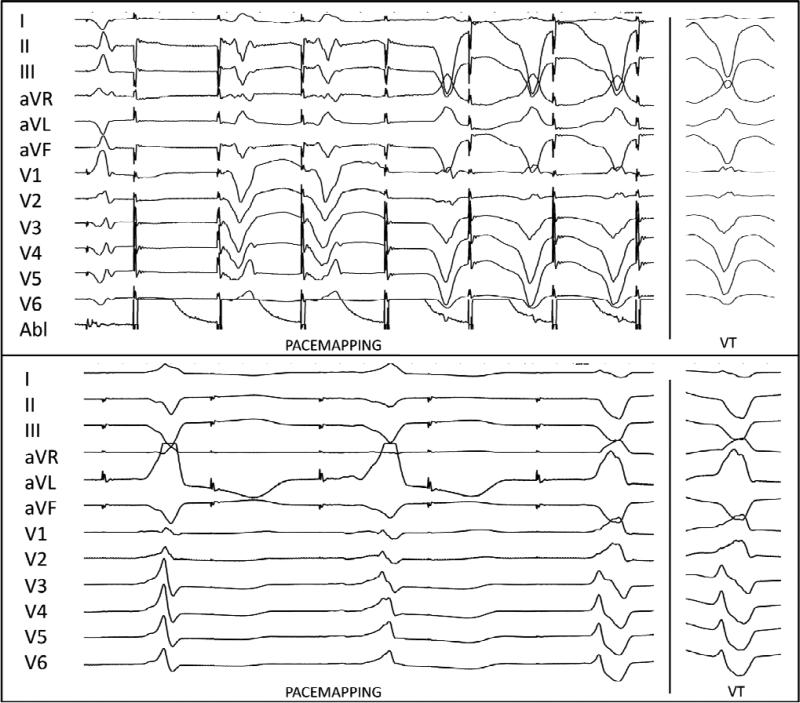
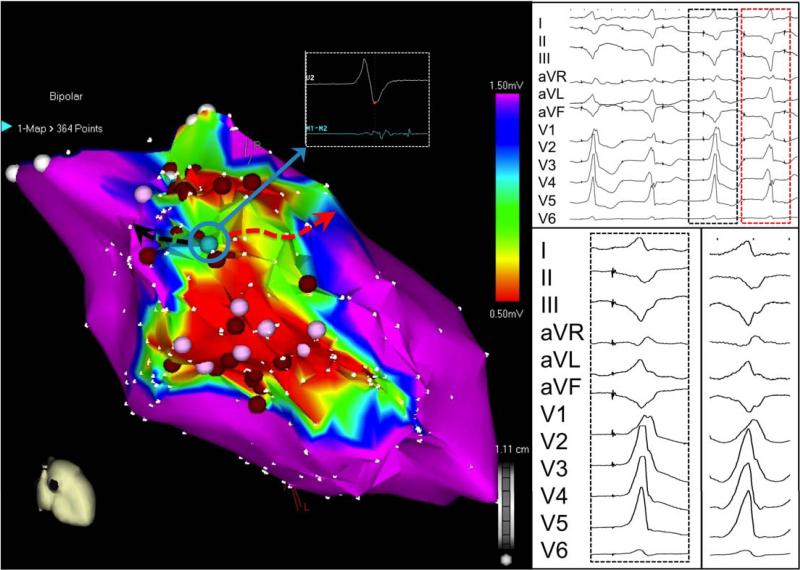
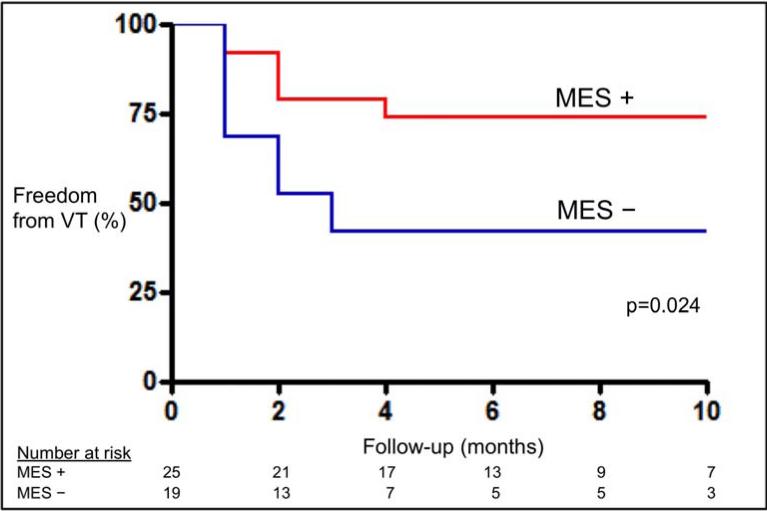
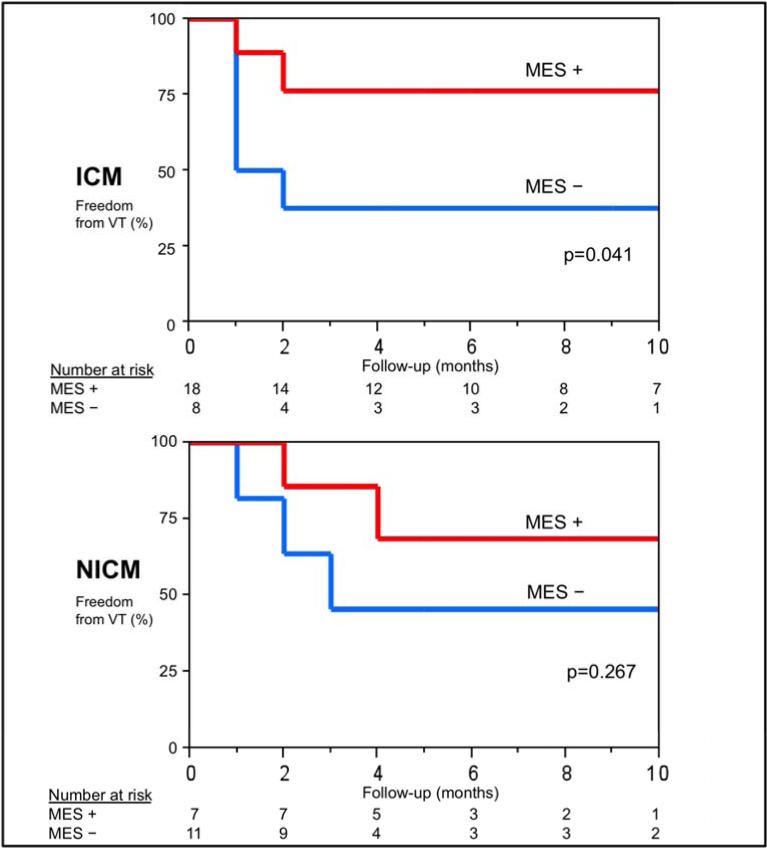
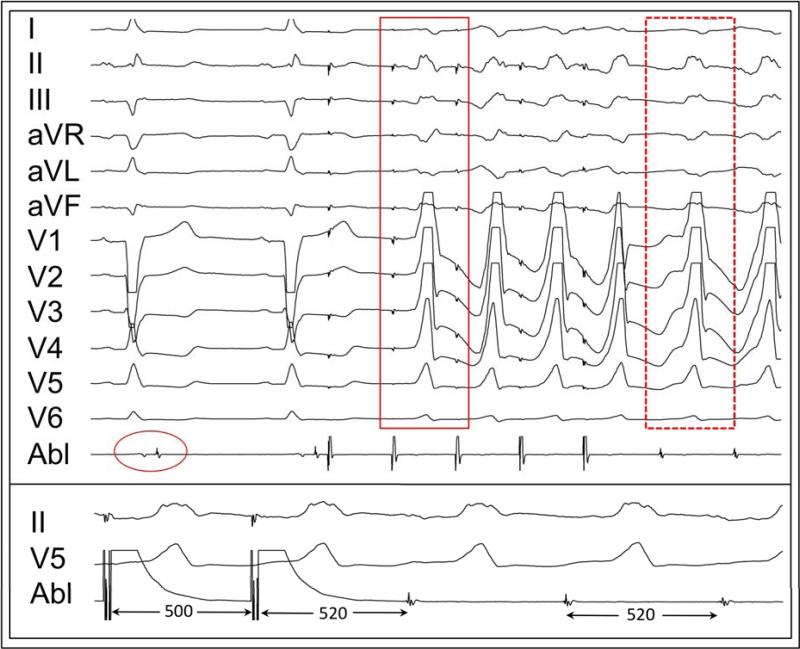
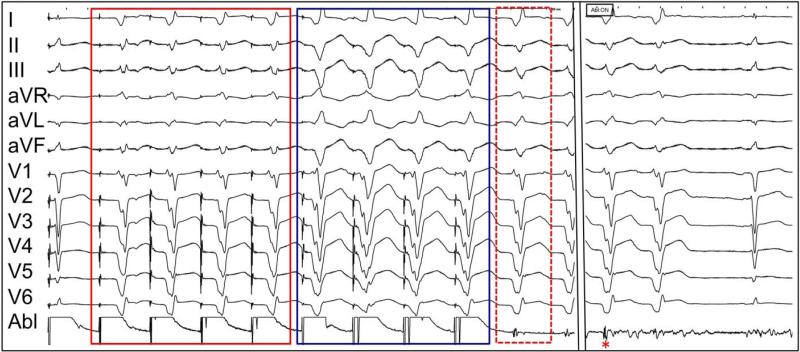
Background: Myocardial scars harbor areas of slow conduction and display abnormal electrograms. Pace-mapping at these sites can generate a 12-lead ECG morphological match to a targeted ventricular tachycardia (VT), and in some instances, multiple exit morphologies can result. At times, this can also result in the initiation of VT, termed pace-mapped induction (PMI). We hypothesized that in patients undergoing catheter ablation of VT, scar substrates with multiple exit sites (MES) identified during pace-mapping have improved freedom from recurrent VT, and PMI of VT predicts successful sites of termination during ablation.
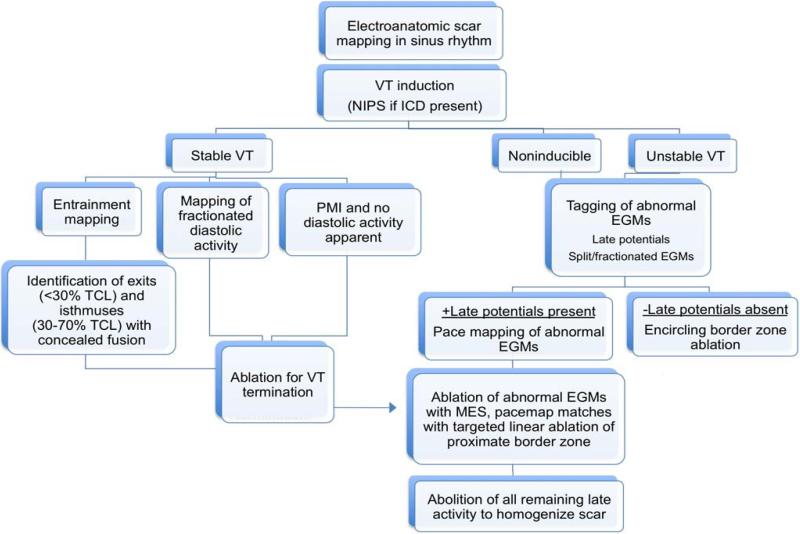
Methods and results: High-density mapping was performed in all subjects to delineate scar (0.5-1.5 mV). Sites with abnormal electrograms were tagged, stimulated (bipolar 10 mA at 2 ms), and targeted for ablation. MES was defined as >1 QRS morphology from a single pacing site. PMI was defined as initiation of VT during pace-mapping (400-600 ms). In a 2-year period, 44 consecutive patients with scar-mediated VT underwent mapping and ablation. MES were observed during pace-mapping in 25 patients (57%). At 9 months, 74% of patients who exhibited MES during pace-mapping had no recurrence of VT compared with 42% of those without MES observed (P=0.024), with an overall freedom from VT of 61%. Thirteen patients (30%) demonstrated PMI, and termination of VT was seen in 95% (18/19) of sites where ablation was performed.
Conclusions: During pace-mapping, electrograms that exhibit MES and PMI may be specific for sites critical to reentry. These functional responses hold promise for identifying important sites for catheter ablation of VT.
Figures
Comment in
-
Letter by Obeyesekere regarding article, "functional pace-mapping responses for identification of targets for catheter ablation of scar-mediated ventricular tachycardia".Circ Arrhythm Electrophysiol. 2012 Oct;5(5):e100; author reply e101. doi: 10.1161/CIRCEP.112.974055. Circ Arrhythm Electrophysiol. 2012. PMID: 23074326 No abstract available.
References
-
- Josephson ME. Electrophysiology of ventricular tachycardia: an historical perspective. J Cardiovasc Electrophysiol. 2003;14:1134–1148. - PubMed
-
- Marchlinski FE, Callans DJ, Gottlieb CD, Zado E. Linear ablation lesions for control of unmappable ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circulation. 2000;101:1288–1296. - PubMed
-
- Soejima K, Suzuki M, Maisel WH, Brunckhorst CB, Delacretaz E, Blier L, Tung S, Khan H, Stevenson WG. Catheter ablation in patients with multiple and unstable ventricular tachycardias after myocardial infarction: short ablation lines guided by reentry circuit isthmuses and sinus rhythm mapping. Circulation. 2001;104:664–669. - PubMed
-
- Bogun F, Good E, Reich S, Elmouchi D, Igic P, Lemola K, Tschopp D, Jongnarangsin K, Oral H, Chugh A, Pelosi F, Morady F. Isolated potentials during sinus rhythm and pace-mapping within scars as guides for ablation of post-infarction ventricular tachycardia. J Am Coll Cardiol. 2006;47:2013–2019. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
