

Disease flare of ankylosing spondylitis presenting as reactive arthritis with seropositivity: a case report
- PMID: 22333429
- PMCID: PMC3295684
- DOI: 10.1186/1752-1947-6-60
Disease flare of ankylosing spondylitis presenting as reactive arthritis with seropositivity: a case report
Abstract
Introduction: Concurrent rheumatoid factor seropositivity is occasionally detected in ankylosing spondylitis and often causes confusion in clinical routine. Overlap between various seronegative arthritides is a known but uncommon association. Differentiation of spondyloarthropathy from rheumatoid arthritis is important, since the natural history, complications, treatments and prognosis of the two diseases differ significantly.
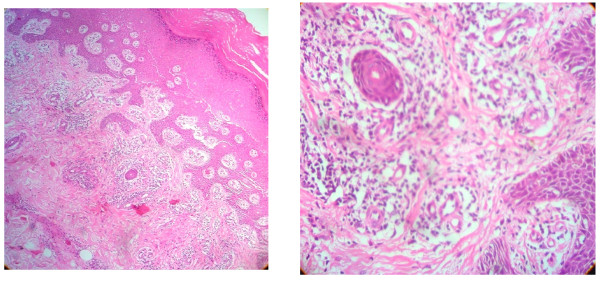
Case presentation: Here, we report the case of a 47-year-old Sri Lankan man who had a long history of intermittent joint pains worsening following a recent episode of self-resolving non-bloody diarrhea. Subsequently, he developed a skin rash suggestive of keratoderma blenorrhagica and circinate balanitis. He had classical radiological evidence of ankylosing spondylosis (previously undiagnosed) associated with human leukocyte antigen B27 antigen, but was positive for rheumatoid factor.
Conclusions: A disease flare of ankylosing spondylitis prompted by a minor diarrheal illness showing well documented features of reactive arthritis is remarkable. The prognostic implications of seropositivity in spondyloarthritis are discussed.
Figures




References
-
- Braun J, Sieper J, Pinucs T. A systematic comparison between rheumatoid arthritis ans ankylosing spondylitis: an introduction. Clin Exp Rheumatol. 2009;27(Suppl 55):1–2. - PubMed
-
- Graham RM. In: Textbook of Dermatology. 5. Burns T, Breathnach S, Cox N, Griffiths C, editor. Oxford, UK: Wiley-Blackwell; 1992. Reiter's disease.
-
- Schneider JM, Mathews JH, Graham BS. Reiter's syndrome. Cutis. 2003;71:198–200. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
