

The cost-effectiveness of routine tuberculosis screening with Xpert MTB/RIF prior to initiation of antiretroviral therapy: a model-based analysis
- PMID: 22333751
- PMCID: PMC3517815
- DOI: 10.1097/QAD.0b013e3283522d47
The cost-effectiveness of routine tuberculosis screening with Xpert MTB/RIF prior to initiation of antiretroviral therapy: a model-based analysis
Abstract
Background: In settings with high tuberculosis (TB) prevalence, 15-30% of HIV-infected individuals initiating antiretroviral therapy (ART) have undiagnosed TB. Such patients are usually screened by symptoms and sputum smear, which have poor sensitivity.
Objective: To project the clinical and economic outcomes of using Xpert MTB/RIF(Xpert), a rapid TB/rifampicin-resistance diagnostic, to screen individuals initiating ART.
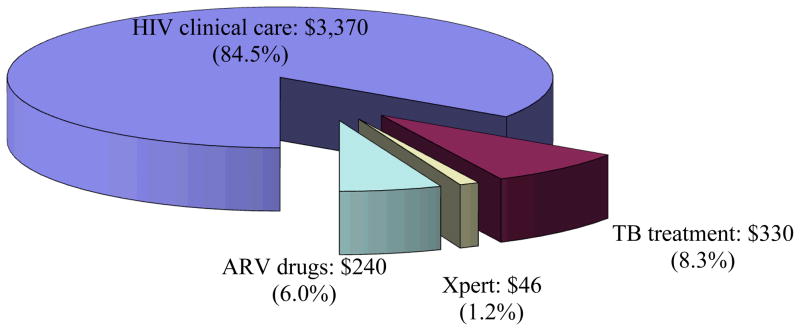
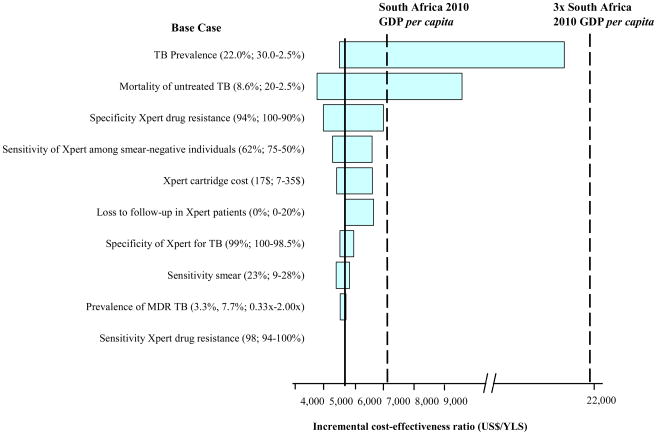
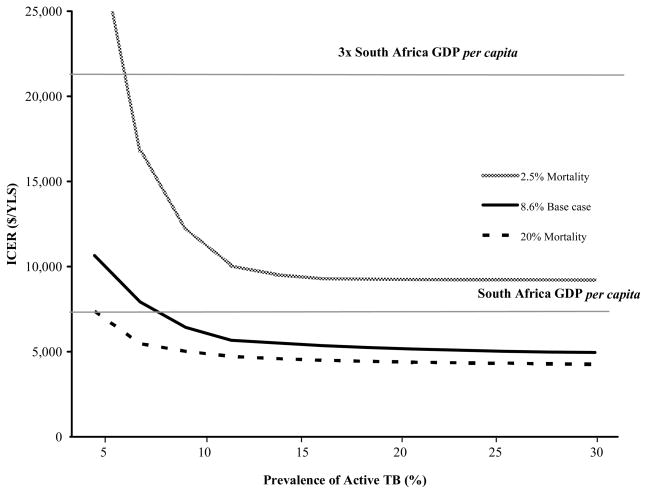
Design: We used a microsimulation model to evaluate the clinical impact and cost-effectiveness of alternative TB screening modalities - in all patients or only symptomatic patients - for hypothetical cohorts of individuals initiating ART in South Africa (mean CD4 cell count = 171 cells/μl; TB prevalence 22%). We simulated no active screening and four diagnostic strategies, smear microscopy (sensitivity 23%); smear and culture (sensitivity, 100%); one Xpert sample (sensitivity in smear-negative TB: 43%); two Xpert samples (sensitivity in smear-negative TB: 62%). Outcomes included projected life expectancy, lifetime costs (2010 US$), and incremental cost-effectiveness ratios (ICERs). Strategies with ICERs less than $7100 (South African gross domestic product per capita) were considered very cost-effective.
Results: Compared with no screening, life expectancy in TB-infected patients increased by 1.6 months using smear in symptomatic patients and by 6.6 months with two Xpert samples in all patients. At 22% TB prevalence, the ICER of smear for all patients was $2800 per year of life saved (YLS), and of Xpert (two samples) for all patients was $5100/YLS. Strategies involving one Xpert sample or symptom screening were less efficient.
Conclusion: Model-based analysis suggests that screening all individuals initiating ART in South Africa with two Xpert samples is very cost-effective.
Figures
References
-
- World Health Organization. Global Tuberculosis Control 2011. Geneva: 2011. [Accessed 9 January 2012]. Available: http://www.who.int/tb/publications/global_report/en/index.html.
-
- Getahun H, Kittikraisak W, Heilig CM, Corbett EL, Ayles H, et al. Development of a standardized screening rule for tuberculosis in people living with HIV in resource-constrained settings: individual participant data meta-analysis of observational studies. PLoS Med. 2011;8:e1000391. doi: 10.1371/journal.pmed.1000391. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
