

Persistent socioeconomic inequalities in cardiovascular risk factors in England over 1994-2008: a time-trend analysis of repeated cross-sectional data
- PMID: 22333887
- PMCID: PMC3342910
- DOI: 10.1186/1471-2458-12-129
Persistent socioeconomic inequalities in cardiovascular risk factors in England over 1994-2008: a time-trend analysis of repeated cross-sectional data
Abstract
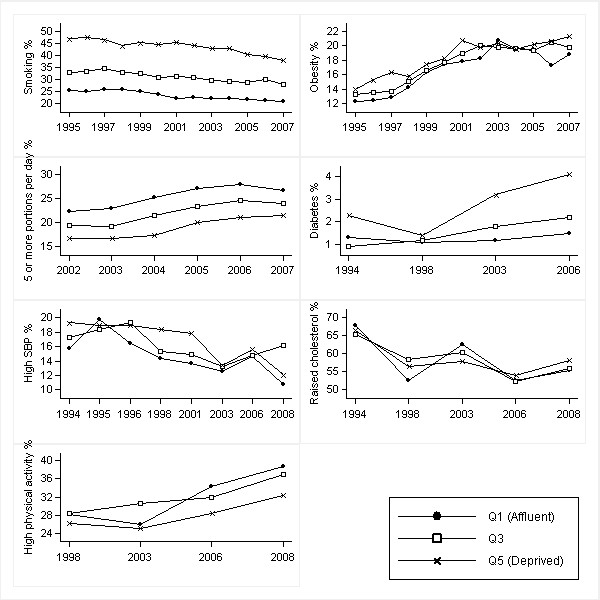
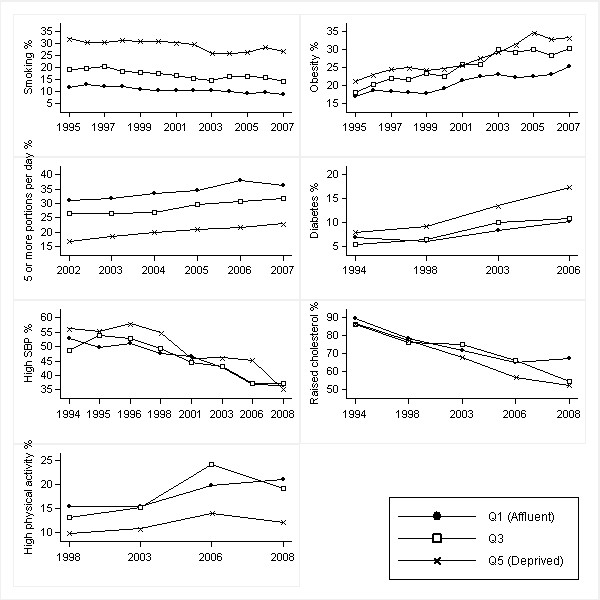
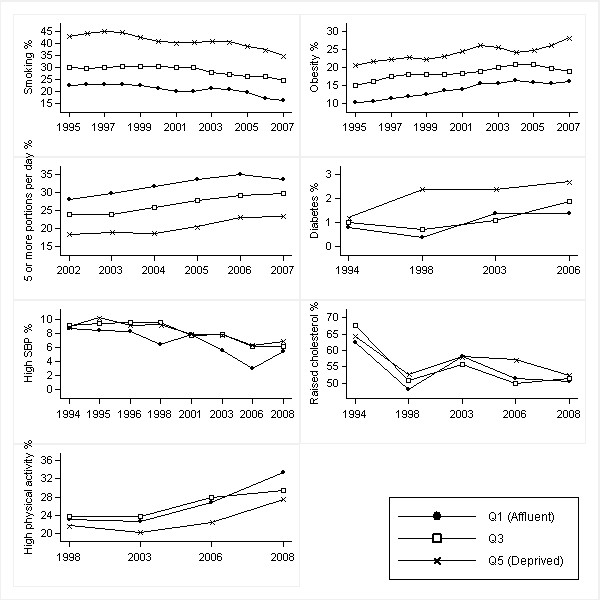
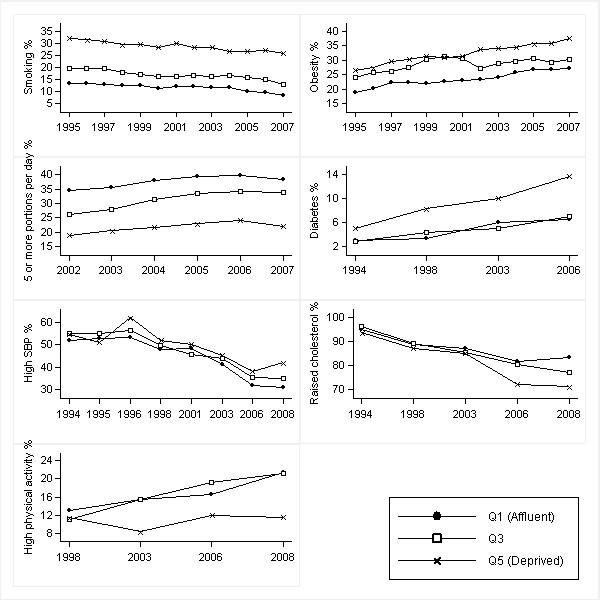
Background: Our aims were to determine the pace of change in cardiovascular risk factors by age, gender and socioeconomic groups from 1994 to 2008, and quantify the magnitude, direction and change in absolute and relative inequalities.
Methods: Time trend analysis was used to measure change in absolute and relative inequalities in risk factors by gender and age (16-54, ≥ 55 years), using repeated cross-sectional data from the Health Survey for England 1994-2008. Seven risk factors were examined: smoking, obesity, diabetes, high blood pressure, raised cholesterol, consumption of five or more daily portions of fruit and vegetables, and physical activity. Socioeconomic group was measured using the Index of Multiple Deprivation 2007.
Results: Between 1994 and 2008, the prevalence of smoking, high blood pressure and raised cholesterol decreased in most deprivation quintiles. However, obesity and diabetes increased. Increasing absolute inequalities were found in obesity in older men and women (p = 0.044 and p = 0.027 respectively), diabetes in young men and older women (p = 0.036 and p = 0.019 respectively), and physical activity in older women (p = 0.025). Relative inequality increased in high blood pressure in young women (p = 0.005). The prevalence of raised cholesterol showed widening absolute and relative inverse gradients from 1998 onwards in older men (p = 0.004 and p ≤ 0.001 respectively) and women (p ≤ 0.001 and p ≤ 0.001).
Conclusions: Favourable trends in smoking, blood pressure and cholesterol are consistent with falling coronary heart disease death rates. However, adverse trends in obesity and diabetes are likely to counteract some of these gains. Furthermore, little progress over the last 15 years has been made towards reducing inequalities. Implementation of known effective population based approaches in combination with interventions targeted at individuals/subgroups with poorer cardiovascular risk profiles are therefore recommended to reduce social inequalities.
Figures
References
-
- Capewell S, Beaglehole R, Seddon M, McMurray JJ. Explanation for the decline in coronary heart disease mortality rates in Auckland, New Zealand, between 1982 and 1993. Circulation. 2000;102:1511–1516. - PubMed
-
- Hunink MGM, Goldman L, Tosteson ANA, Mittleman MA, Goldman PA, Williams LW, Tsevat J, Weinstein MC. The recent decline in mortality from coronary heart disease, 1980-1990. The effect of secular trends in risk factors and treatments. JAMA. 1997;277:535–542. doi: 10.1001/jama.1997.03540310033031. - DOI - PubMed
-
- Kaplan GA, Keil JE. Socioeconomic factors and cardiovascular disease: a review of the literature. Circulation. 1993;88:1973–1988. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
