

Effects of mometasone furoate/formoterol fumarate fixed-dose combination formulation on chronic obstructive pulmonary disease (COPD): results from a 52-week Phase III trial in subjects with moderate-to-very severe COPD
- PMID: 22334769
- PMCID: PMC3276257
- DOI: 10.2147/COPD.S27320
Effects of mometasone furoate/formoterol fumarate fixed-dose combination formulation on chronic obstructive pulmonary disease (COPD): results from a 52-week Phase III trial in subjects with moderate-to-very severe COPD
Abstract
Rationale: The purpose of this study was to investigate the clinical efficacy and safety of a fixed-dose combination of mometasone furoate/formoterol fumarate (MF/F) administered via a metered-dose inhaler in subjects with moderate-to-very severe chronic obstructive pulmonary disease (COPD).
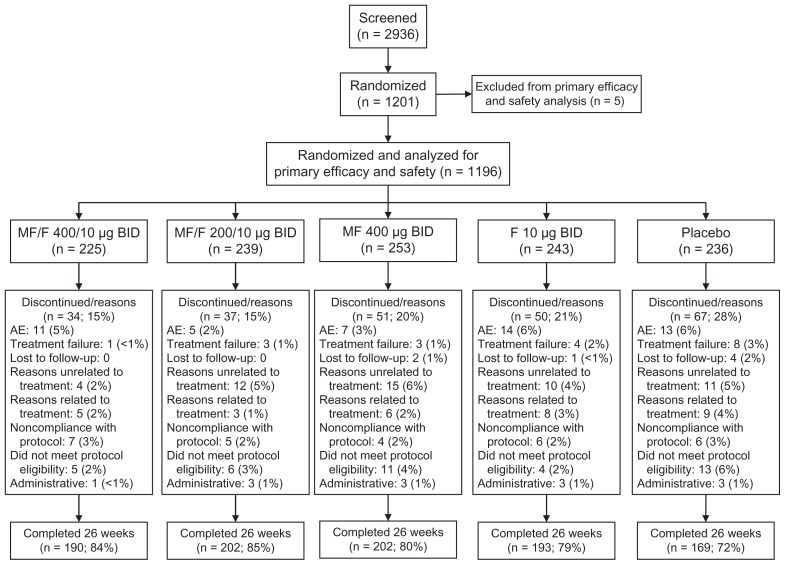
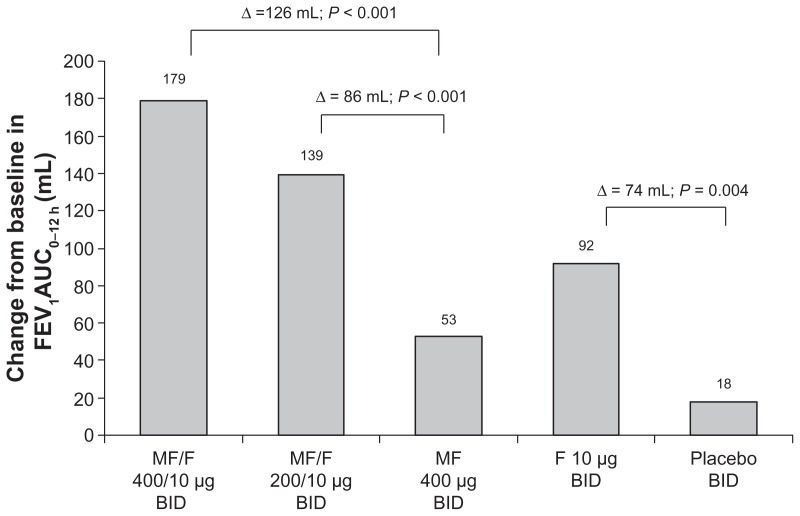
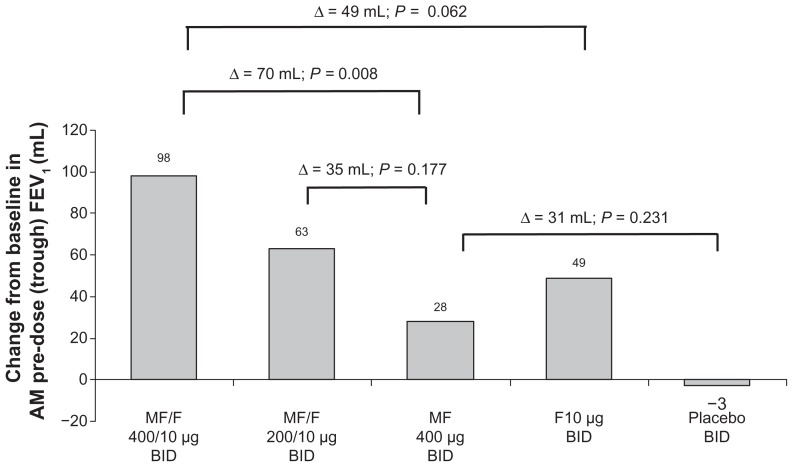
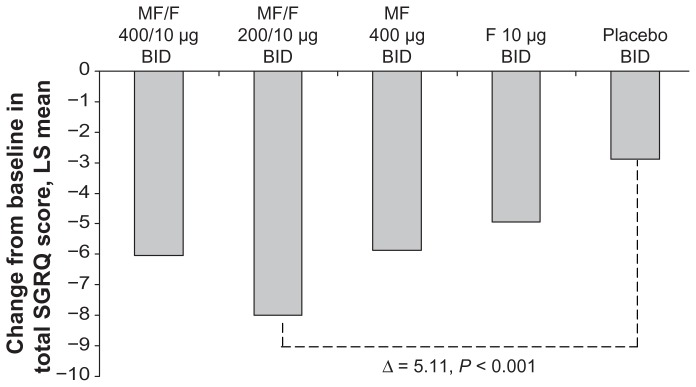
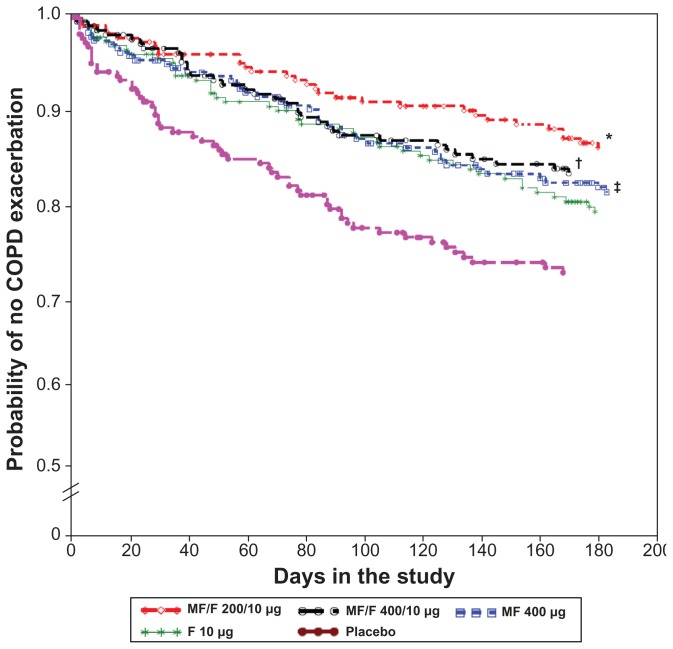
Methods: This multicenter, double-blind, placebo-controlled trial had a 26-week treatment period and a 26-week safety extension. Subjects (n = 1196), at least 40 years old, were current or ex-smokers randomized to twice-daily inhaled MF/F 400/10 μg, MF/F 200/10 μg, MF 400 μg, F 10 μg, or placebo. The trial's co-primary endpoints were mean changes from baseline, as area under the curve (AUC), in forced expiratory volume (FEV(1)) over 0-12 hours (AUC(0-12 h) FEV(1)) with MF/F versus MF, and in morning (AM) pre-dose (trough) FEV(1) with MF/F versus F after 13 weeks of treatment. Key secondary endpoints were the effects of MF/F on respiratory health status using the Saint George's Respiratory Questionnaire (SGRQ), symptom-free nights, partly stable COPD at 26 weeks, and time to first COPD exacerbation.
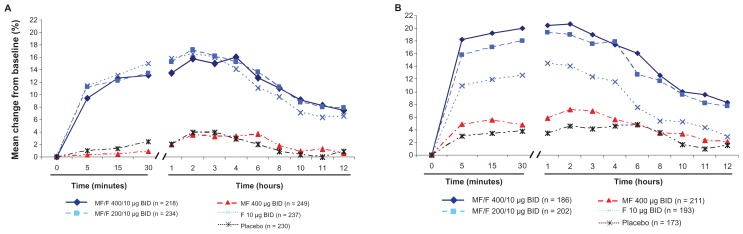
Results: The largest improvements in AUC(0-12 h) FEV(1) were observed with MF/F 400/10 μg and MF/F 200/10 μg. Serial spirometry results demonstrated that bronchodilator effects with MF/F occurred rapidly (within 5 minutes), persisted for 12 hours after dosing, and were sustained over the 26-week treatment period. Similar findings were observed for AM pre-dose FEV(1), for which effects were further investigated, excluding subjects whose AM FEV(1) data were incorrectly collected after 2 days from the last dose of study treatment. Improvements in SGRQ scores surpassed the minimum clinically important difference of more than four units with both MF/F treatments. At 26 weeks, no notable between-treatment differences in the occurrence and nature of adverse events (AEs) were reported. No unexpected AEs were observed. Overall, 90 subjects reported AEs considered to be treatment-related, the most common of which were lenticular opacities, dysphonia, and oral candidiasis.
Discussion: In conclusion, MF/F treatments improved lung function and respiratory health status, reduced exacerbations, and were well tolerated in subjects with moderate-to-very severe COPD.
Trial registration: ClinicalTrials.gov NCT00383721.
Keywords: COPD; FEV1; bronchodilator; exacerbation; inhaled corticosteroid; spirometry.
Figures
References
-
- American College of Physicians. Four physician organizations issue new clinical recommendations for diagnosing and treating COPD. [Accessed August 4, 2011]. Available at: http://www.acponline.org/pressroom/copd_clinical_recommendations.htm.
-
- Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23:932–946. - PubMed
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) Global strategy for the diagnosis, management and prevention of COPD. [Accessed July 21, 2011]. Available at: http://www.goldcopd.org/
-
- Donohue JF. Therapeutic responses in asthma and COPD. Bronchodilators. Chest. 2004;126:125S–137S. discussion 159S–161S. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
