

Randomized, double-blind clinical trial of two different modes of positive airway pressure therapy on adherence and efficacy in children
- PMID: 22334807
- PMCID: PMC3266335
- DOI: 10.5664/jcsm.1656
Randomized, double-blind clinical trial of two different modes of positive airway pressure therapy on adherence and efficacy in children
Abstract
Study objectives: To determine the effects of bilevel positive airway pressure with pressure release technology (Bi-Flex) on adherence and efficacy in children and adolescents compared to standard continuous positive airway pressure (CPAP) therapy. We hypothesized that Bi-Flex would result in improved adherence but similar efficacy to CPAP.
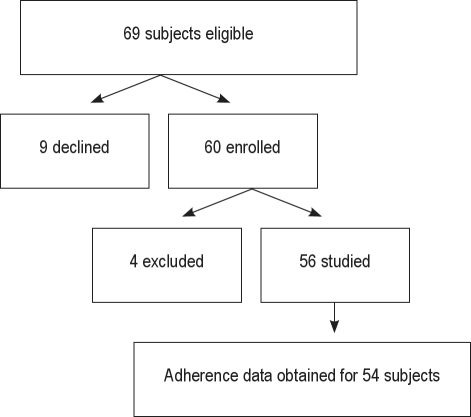
Methods: This was a randomized, double-blinded clinical trial. Patients with obstructive sleep apnea were randomized to CPAP or Bi-Flex. Repeat polysomnography was performed on pressure at 3 months. Objective adherence data were obtained at 1 and 3 months.
Results: 56 children and adolescents were evaluated. There were no significant differences in the number of nights the device was turned on, or the mean number of minutes used at pressure per night for CPAP vs Bi-Flex (24 ± 6 vs 22 ± 9 nights, and 201 ± 135 vs 185 ± 165 min, respectively, for Month 1). The apnea hypopnea index decreased significantly from 22 ± 21/h to 2 ± 3/h on CPAP (p = 0.005), and 18 ± 15/h to 2 ± 2/h on Bi-Flex (p < 0.0005), but there was no significant difference between groups (p = 0.82 for CPAP vs Bi-Flex). The Epworth Sleepiness Scale decreased from 8 ± 5 to 6 ± 3 on CPAP (p = 0.14), and 10 ± 6 to 5 ± 5 on Bi-Flex (p < 0.0005; p = 0.12 for CPAP vs Bi-Flex).
Conclusions: Both CPAP and Bi-Flex are efficacious in treating children and adolescents with OSAS. However, adherence is suboptimal with both methods. Further research is required to determine ways to improve adherence in the pediatric population.
Keywords: Bi-Flex; CPAP; obstructive sleep apnea.
Figures
Comment in
-
The quest to improve CPAP adherence--PAP potpourri is not the answer.J Clin Sleep Med. 2012 Feb 15;8(1):49-50. doi: 10.5664/jcsm.1660. J Clin Sleep Med. 2012. PMID: 22334809 Free PMC article. No abstract available.
References
-
- American Academy of Pediatrics. Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2002;109:704–12. - PubMed
-
- Marcus CL, Rosen G, Ward SL, et al. Adherence to and effectiveness of positive airway pressure therapy in children with obstructive sleep apnea. Pediatrics. 2006;117:e442–51. - PubMed
-
- O'Donnell AR, Bjornson CL, Bohn SG, Kirk VG. Compliance rates in children using noninvasive continuous positive airway pressure. Sleep. 2006;29:651–8. - PubMed
-
- Uong EC, Epperson M, Bathon SA, Jeffe DB. Adherence to nasal positive airway pressure therapy among school-aged children and adolescents with obstructive sleep apnea syndrome. Pediatrics. 2007;120:e1203–11. - PubMed
-
- Reeves-Hoche MK, Hudgel DW, Meck R, Witteman R, Ross A, Zwillich CW. Continuous versus bilevel positive airway pressure for obstructive sleep apnea. Am J Respir Crit Care Med. 1995;151:443–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
