Impact of birth rate, seasonality and transmission rate on minimum levels of coverage needed for rubella vaccination
- PMID: 22335852
- PMCID: PMC3487482
- DOI: 10.1017/S0950268812000131
Impact of birth rate, seasonality and transmission rate on minimum levels of coverage needed for rubella vaccination
Abstract
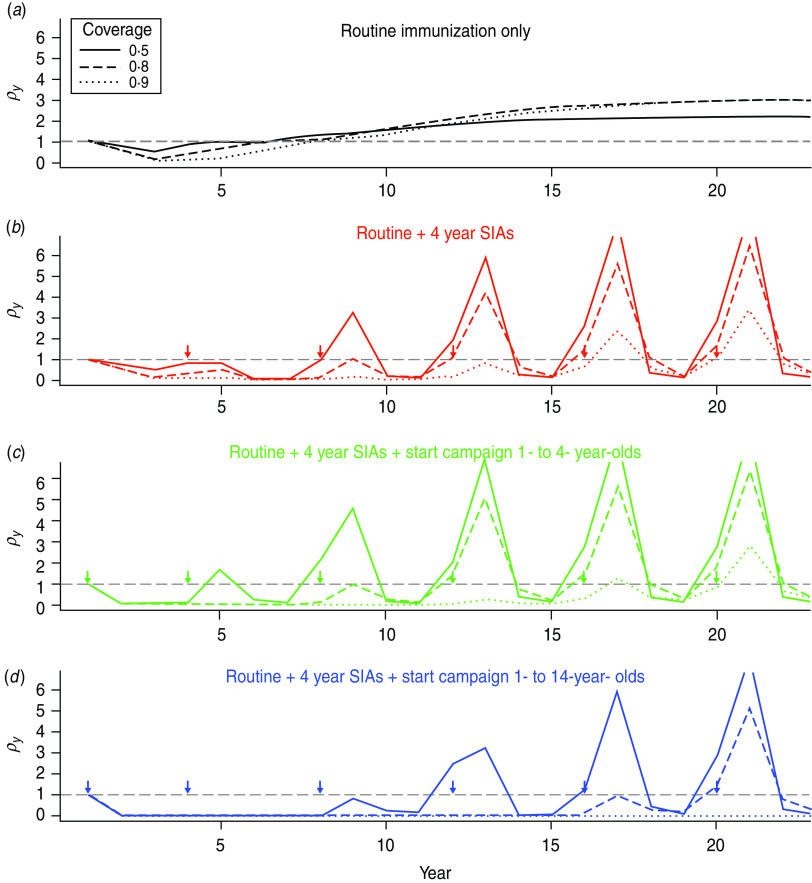
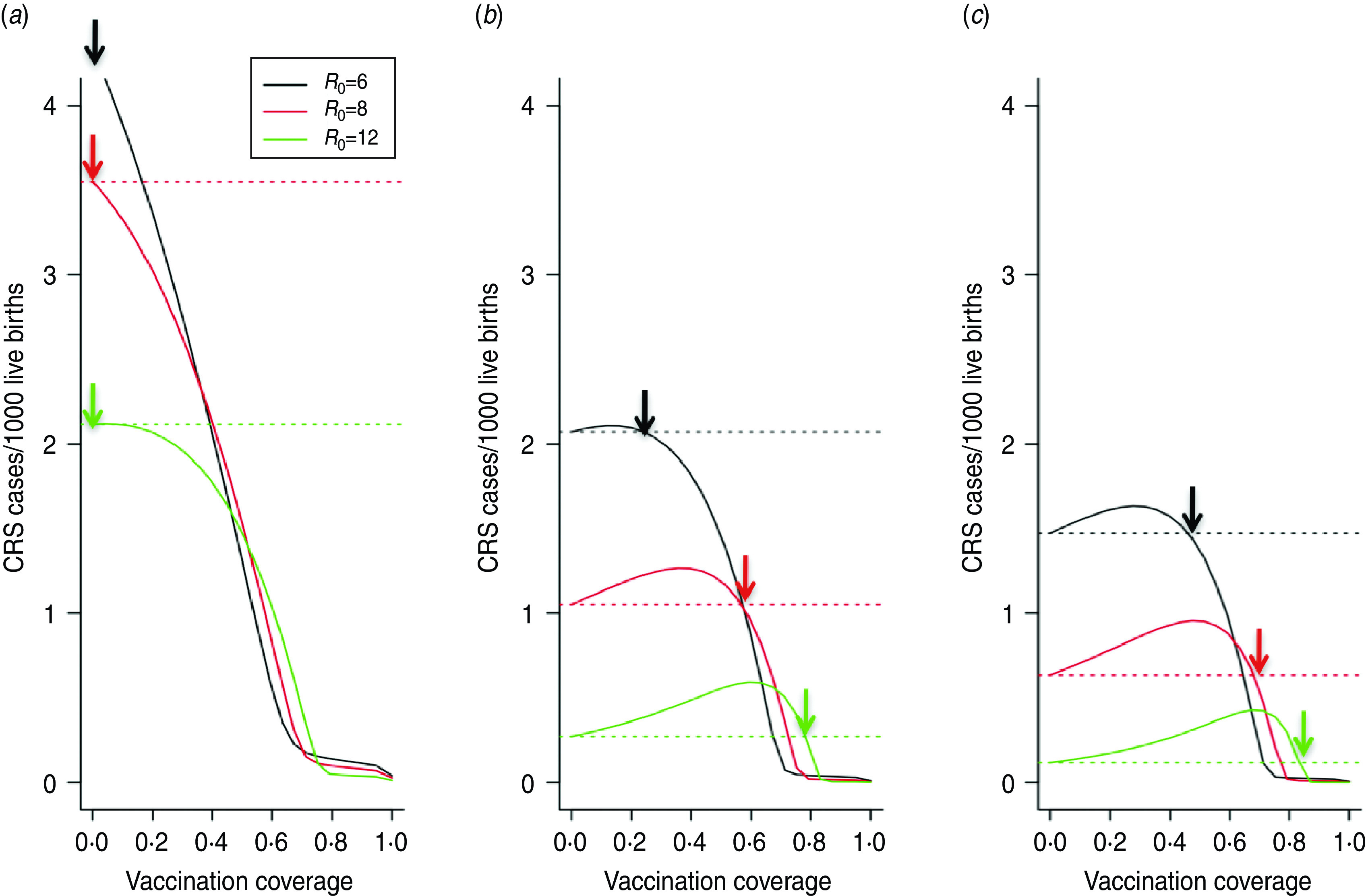
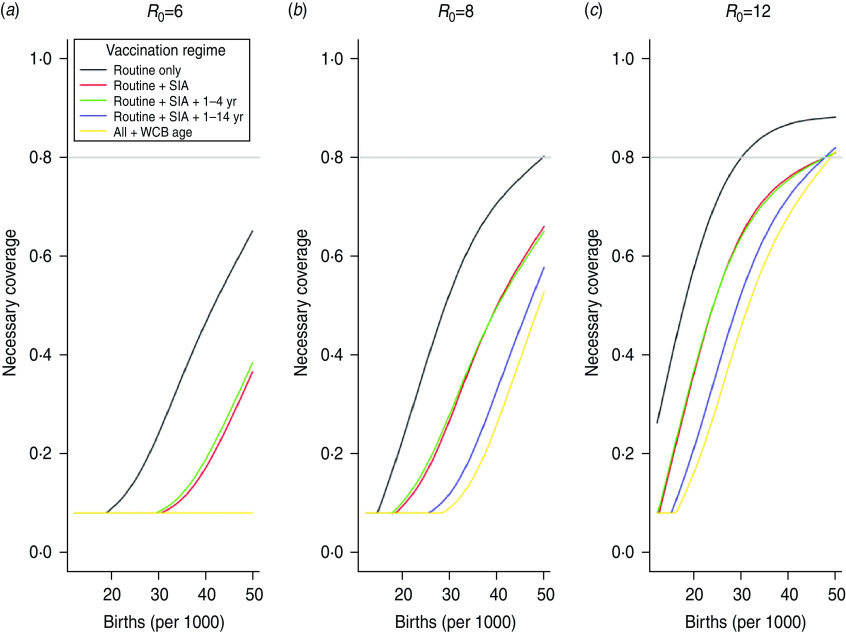
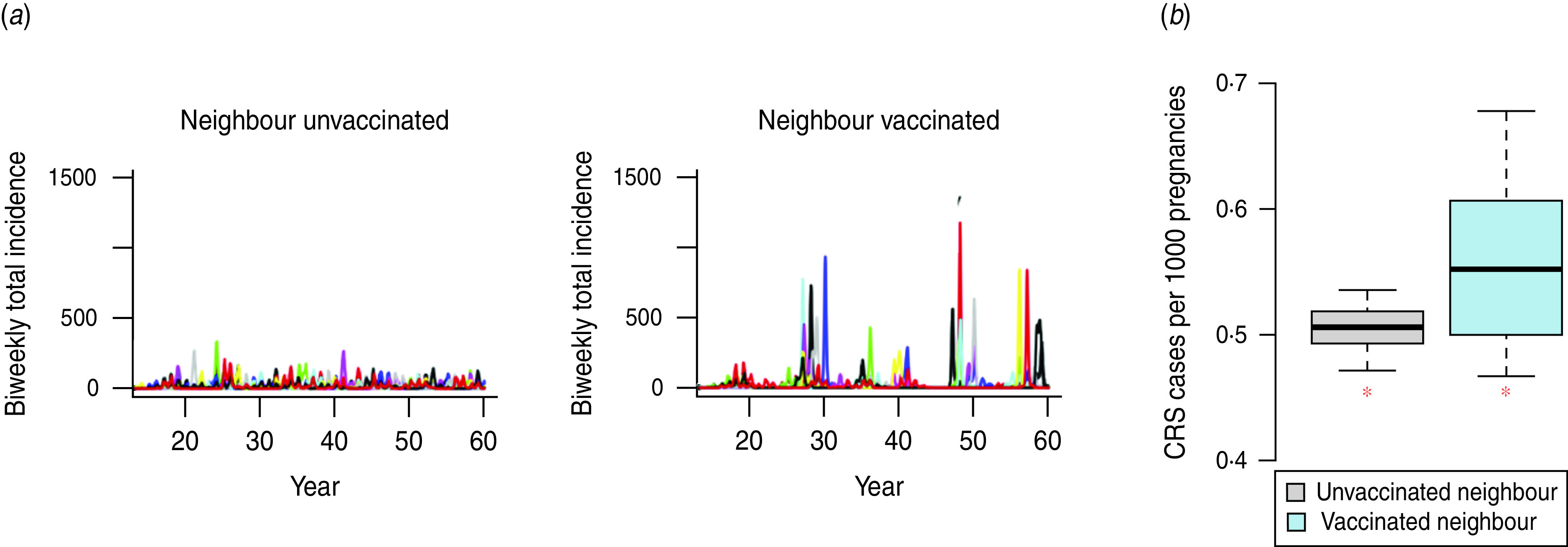
Childhood rubella infection in early pregnancy can lead to fetal death or congenital rubella syndrome (CRS) with multiple disabilities. Reduction of transmission via universal vaccination can prevent CRS, but inadequate coverage may increase CRS numbers by increasing the average age at infection. Consequently, many countries do not vaccinate against rubella. The World Health Organization recommends that for safe rubella vaccination, at least 80% coverage of each birth cohort should be sustained. The nonlinear relationship between CRS burden and infection dynamics has been much studied; however, how the complex interaction between epidemic and demographic dynamics affects minimum safe levels of coverage has not been quantitatively evaluated across scales necessary for a global assessment. We modelled 30-year CRS burdens across epidemiological and demographic settings, including the effect of local interruption of transmission via stochastic fadeout. Necessary minimum vaccination coverage increases markedly with birth and transmission rates, independent of amplitude of seasonal fluctuations in transmission. Susceptible build-up in older age groups following local stochastic extinction of rubella increased CRS burden, indicating that spatial context is important. In low birth-rate settings, 80% routine coverage is a conservative guideline, particularly if supplemented with campaigns and vaccination of women of childbearing age. Where birth and transmission rates are high, immunization coverage must be well above 80% and campaigns may be needed. Policy-makers should be aware of the potential negative effect of local extinction of rubella, since heterogeneity in vaccination coverage will shape extinction patterns, potentially increasing CRS burdens.
Figures
Similar articles
-
Balancing evidence and uncertainty when considering rubella vaccine introduction.PLoS One. 2013 Jul 5;8(7):e67639. doi: 10.1371/journal.pone.0067639. Print 2013. PLoS One. 2013. PMID: 23861777 Free PMC article.
-
The impact of sub-national heterogeneities in demography and epidemiology on the introduction of rubella vaccination programs in Nigeria.Vaccine. 2024 Aug 13;42(20):125982. doi: 10.1016/j.vaccine.2024.05.030. Epub 2024 May 29. Vaccine. 2024. PMID: 38811269 Free PMC article.
-
Congenital rubella syndrome: a matter of concern.Rev Panam Salud Publica. 2015 Mar;37(3):179-86. Rev Panam Salud Publica. 2015. PMID: 25988255 Review.
-
Informing rubella vaccination strategies in East Java, Indonesia through transmission modelling.Vaccine. 2016 Nov 4;34(46):5636-5642. doi: 10.1016/j.vaccine.2016.09.010. Epub 2016 Sep 23. Vaccine. 2016. PMID: 27670077
-
Congenital rubella syndrome: A brief review of public health perspectives.Indian J Public Health. 2018 Jan-Mar;62(1):52-54. doi: 10.4103/ijph.IJPH_275_16. Indian J Public Health. 2018. PMID: 29512566 Review.
Cited by
-
Introduction of rubella-containing-vaccine to Madagascar: implications for roll-out and local elimination.J R Soc Interface. 2016 Apr;13(117):20151101. doi: 10.1098/rsif.2015.1101. J R Soc Interface. 2016. PMID: 27122178 Free PMC article.
-
Estimates of the global burden of Congenital Rubella Syndrome, 1996-2019.Int J Infect Dis. 2023 Dec;137:149-156. doi: 10.1016/j.ijid.2023.09.003. Epub 2023 Sep 9. Int J Infect Dis. 2023. PMID: 37690575 Free PMC article.
-
Strategies for elimination of rubella in pregnancy and of congenital rubella syndrome in high and upper-middle income countries.J Prev Med Hyg. 2020 Apr 2;61(1):E98-E108. doi: 10.15167/2421-4248/jpmh2020.61.1.1310. eCollection 2020 Mar. J Prev Med Hyg. 2020. PMID: 32490275 Free PMC article. Review.
-
Computational modeling of interventions and protective thresholds to prevent disease transmission in deploying populations.Comput Math Methods Med. 2014;2014:785752. doi: 10.1155/2014/785752. Epub 2014 Jun 9. Comput Math Methods Med. 2014. PMID: 25009579 Free PMC article.
-
Development and dissemination of infectious disease dynamic transmission models during the COVID-19 pandemic: what can we learn from other pathogens and how can we move forward?Lancet Digit Health. 2021 Jan;3(1):e41-e50. doi: 10.1016/S2589-7500(20)30268-5. Epub 2020 Dec 7. Lancet Digit Health. 2021. PMID: 33735068 Free PMC article. Review.
References
-
- Gregg NM. Congenital defects associated with maternal rubella. The Australian Hospital 1947; 14: 7–9. - PubMed
-
- World Health Organization.Rubella vaccines: WHO position paper. Weekly Epidemiological Record 2011; 86: 301–316.
-
- Anderson RM, May RM. Vaccination and herd immunity to infectious diseases. Nature 1985; 318: 323–329. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical