

Survival after chemotherapy and/or radiotherapy versus self-expanding metal stent insertion in the setting of inoperable esophageal cancer: a case-control study
- PMID: 22336151
- PMCID: PMC3305548
- DOI: 10.1186/1471-2407-12-70
Survival after chemotherapy and/or radiotherapy versus self-expanding metal stent insertion in the setting of inoperable esophageal cancer: a case-control study
Abstract
Background: Our aim was to compare survival of the various treatment modality groups of chemotherapy and/or radiotherapy in relation to SEMS (self-expanding metal stents) in a retrospective case-control study. We have made the hypothesis that the administration of combined chemoradiotherapy improves survival in inoperable esophageal cancer patients.
Methods: All patients were confirmed histologically as having surgically non- resectable esophageal carcinoma. Included were patients with squamous cell carcinoma, undifferentiated carcinoma as well as Siewert type I--but not type II - esophagogastric junctional adenocarcinoma. The decision to proceed with palliative treatments was taken within the context of a multidisciplinary team meeting and full expert review based on patient's wish, co-morbid disease, clinical metastases, distant metastases, M1 nodal metastases, T4-tumor airway, aorta, main stem bronchi, cardiac invasion, and peritoneal disease. Patients not fit enough to tolerate a radical course of definitive chemo- and/or radiation therapy were referred for self-expanding metal stent insertion. Our approach to deal with potential confounders was to match subjects according to their clinical characteristics (contraindications for surgery) and tumor stage according to diagnostic work-up in four groups: SEMS group (A), Chemotherapy group (B), Radiotherapy group (C), and Chemoradiotherapy group (D).
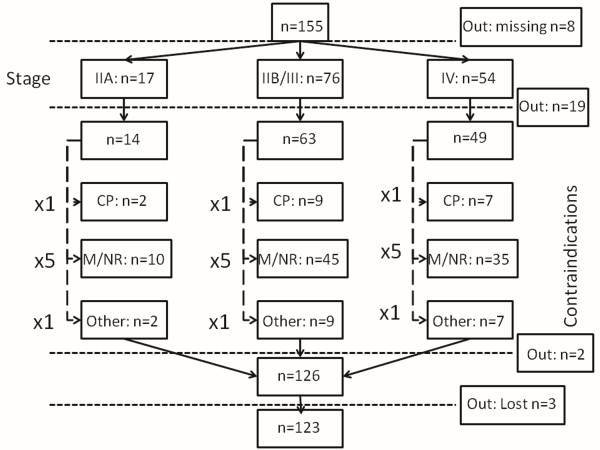
Results: Esophagectomy was contraindicated in 155 (35.5%) out of 437 patients presenting with esophageal cancer to the Department of General and Abdominal Surgery of the University Hospital of Mainz, Germany, between November 1997 and November 2007. There were 133 males and 22 females with a median age of 64.3 (43-88) years. Out of 155 patients, 123 were assigned to four groups: SEMS group (A) n = 26, Chemotherapy group (B) n = 12, Radiotherapy group (C) n = 23 and Chemoradiotherapy group (D) n = 62. Mean patient survival for the 4 groups was as follows: Group A: 6.92 ± 8.4 months; Group B: 7.75 ± 6.6 months; Group C: 8.56 ± 9.5 months, and Group D: 13.53 ± 14.7 months. Significant differences in overall survival were associated with tumor histology (P = 0.027), tumor localization (P = 0.019), and type of therapy (P = 0.005), respectively, in univariate analysis. Treatment modality (P = 0.043) was the only independent predictor of survival in multivariate analysis. The difference in overall survival between Group A and Group D was highly significant (P < 0.01) and in favor of Group D. As concerns Group D versus Group B and Group D versus Group C there was a trend towards a difference in overall survival in favor of Group D (P = 0.069 and P = 0.059, respectively).
Conclusions: The prognosis of inoperable esophageal cancer seems to be highly dependent on the suitability of the induction of patient-specific therapeutic measures and is significantly better, when chemoradiotherapy is applied.
Figures

References
-
- Homs MY, Steyerberg EW, Eijkenboom WM. et al. Palliative treatment of esophageal cancer with dysphagia: more favourable outcome from single-dose internal brachytherapy than from the placement of a self-expanding stent; a multicenter randomised study. Ned Tijdschr Geneeskd. 2005;149:2800–2806. - PubMed
-
- Shenfine J, McNamee P, Steen N. et al. A pragmatic randomised controlled trial of the cost-effectiveness of palliative therapies for patients with inoperable oesophageal cancer. Health Technol Assess. 2005;9:1–121. - PubMed
-
- Bergquist H, Wenger U, Johnsson E. et al. Stent insertion or endoluminal brachytherapy as palliation of patients with advanced cancer of the esophagus and gastroesophageal junction. Results of a randomized, controlled clinical trial. Dis Esophagus. 2005;18:131–139. doi: 10.1111/j.1442-2050.2005.00467.x. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
