

Early use of imipenem/cilastatin and vancomycin followed by de-escalation versus conventional antimicrobials without de-escalation for patients with hospital-acquired pneumonia in a medical ICU: a randomized clinical trial
- PMID: 22336530
- PMCID: PMC3396273
- DOI: 10.1186/cc11197
Early use of imipenem/cilastatin and vancomycin followed by de-escalation versus conventional antimicrobials without de-escalation for patients with hospital-acquired pneumonia in a medical ICU: a randomized clinical trial
Abstract
Introduction: Although early use of broad-spectrum antimicrobials in critically ill patients may increase antimicrobial adequacy, uncontrolled use of these agents may select for more-resistant organisms. This study investigated the effects of early use of broad-spectrum antimicrobials in critically ill patients with hospital-acquired pneumonia.
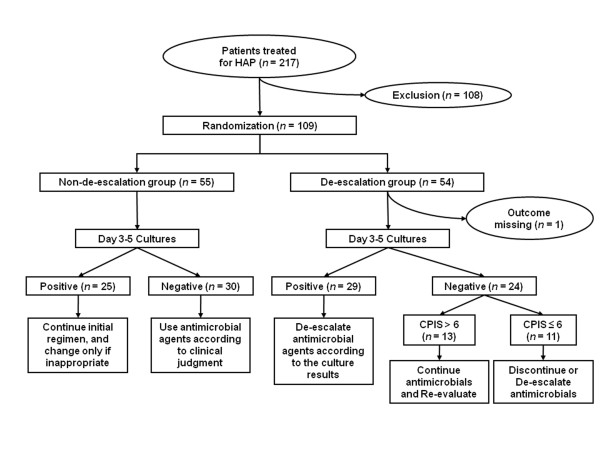
Methods: We compared the early use of broad-spectrum antimicrobials plus subsequent de-escalation (DE) with conventional antimicrobial treatment (non-de-escalation, NDE) in critically ill patients with hospital-acquired pneumonia (HAP). This open-label, randomized clinical trial was performed in patients in a tertiary-care center medical intensive care unit (MICU) in Korea. Patients (n=54) randomized to the DE group received initial imipenem/cilastatin plus vancomycin with subsequent de-escalation according to culture results, whereas patients randomized to the NDE group (n=55) received noncarbapenem, nonvancomycin empiric antimicrobials.
Results: Between November 2004 and October 2006, 109 MICU patients with HAP were enrolled. Initial antimicrobial adequacy was significantly higher in the DE than in the NDE group for Gram-positive organisms (100% versus 14.3%; P<0.001), but not for Gram-negative organisms (64.3% versus 85.7%; P=0.190). Mean intensive care unit (ICU) stay, and 14-day, 28-day, and overall mortality rates did not differ in the two groups. Among culture-positive patients, mortality from methicillin-resistant Staphylococcus aureus (MRSA) pneumonia was higher in the DE group, even after early administration of vancomycin. Multidrug-resistant organisms, especially MRSA, were more likely to emerge in the DE group (adjusted hazard ratio for emergence of MRSA, 3.84; 95% confidence interval, 1.06 to 13.91).
Conclusions: The therapeutic advantage of early administration of broad-spectrum antimicrobials, especially with vancomycin, was not evident in this study.
Figures
References
-
- Trouillet JL, Chastre J, Vuagnat A, Joly-Guillou ML, Combaux D, Dombret MC, Gibert C. Ventilator-associated pneumonia caused by potentially drug-resistant bacteria. Am J Respir Crit Care Med. 1998;157:531–539. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
