

Correction of subclinical coagulation disorders before percutaneous dilatational tracheotomy
- PMID: 22337277
- PMCID: PMC3320783
- DOI: 10.2450/2012.0086-11
Correction of subclinical coagulation disorders before percutaneous dilatational tracheotomy
Abstract
Background: There is evidence that percutaneous dilatational tracheotomy (PDT) can be safely performed in patients with severe coagulation disorders if these are carefully corrected immediately before the procedure. However, it is currently unclear whether PDT can be performed safely in patients in an Intensive Care Unit (ICU) with uncorrected mild coagulation disorders.
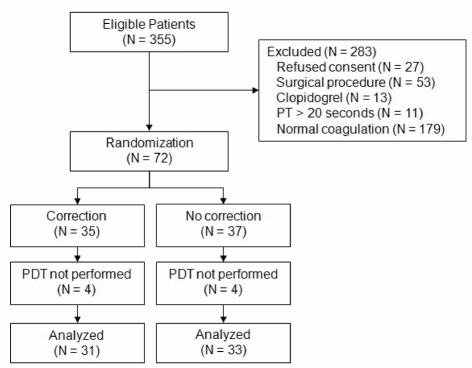
Materials and methods: In a randomised controlled trial we determined the effect of correction of mild coagulation disorders on bleeding during and after PDT. ICU patients planned for bedside PDT with: (i) a prothrombin time (PT) between 14.7-20.0 seconds, (ii) a platelet count between 40-100×10(9)/L and/or (iii) active treatment with acetylsalicylic acid were randomised to receive infusion with fresh-frozen plasma (FFP) and/or platelets ("correction") versus no transfusion ("no correction") before PDT.
Results: We randomised 35 patients to the "correction" group and 37 patients to the "no correction" group. In patients who received FFP, the decrease in PT was marginal (mean decrease 0.40±0.56 seconds); the median increase in platelet counts after transfusion of platelets was 35 [11-47]x10(9)/L. The median blood loss was 3 [IQR: 1-6] grams in the "correction" group and 3 [IQR: 2-6] grams in the "no correction" group (P=0.96).
Discussion: Bleeding during and after bedside PDT in ICU patients with mild coagulation disorders is rare in our setting. Correction of subclinical coagulation disorders by transfusion of FFP and/or platelets does not affect bleeding.
Figures
Similar articles
-
Effect of fresh-frozen plasma transfusion on prothrombin time and bleeding in patients with mild coagulation abnormalities.Transfusion. 2006 Aug;46(8):1279-85. doi: 10.1111/j.1537-2995.2006.00891.x. Transfusion. 2006. PMID: 16934060
-
Coagulation disorders do not increase the risk for bleeding during percutaneous dilatational tracheotomy.Thorac Cardiovasc Surg. 2013 Apr;61(3):234-9. doi: 10.1055/s-0032-1322608. Epub 2013 Jan 23. Thorac Cardiovasc Surg. 2013. PMID: 23344764
-
A survey of physicians' reasons to transfuse plasma and platelets in the critically ill: a prospective single-centre cohort study.Transfus Med. 2009 Aug;19(4):207-12. doi: 10.1111/j.1365-3148.2009.00928.x. Transfus Med. 2009. PMID: 19706138
-
Endoscopic percutaneous dilatational tracheotomy: a prospective evaluation of 500 consecutive cases.Laryngoscope. 2005 Oct;115(10 Pt 2):1-30. doi: 10.1097/01.MLG.0000163744.89688.E8. Laryngoscope. 2005. PMID: 16227862 Review.
-
Critical issues in hematology: anemia, thrombocytopenia, coagulopathy, and blood product transfusions in critically ill patients.Clin Chest Med. 2003 Dec;24(4):607-22. doi: 10.1016/s0272-5231(03)00100-x. Clin Chest Med. 2003. PMID: 14710693 Review.
Cited by
-
Safety Analysis of Visual Percutaneous Tracheostomy in Neurocritical Care Patients with Anticoagulation and Antithrombosis.Neurocrit Care. 2025 Aug;43(1):290-297. doi: 10.1007/s12028-024-02191-z. Epub 2025 Jan 17. Neurocrit Care. 2025. PMID: 39825159
-
Transfusion strategies in non-bleeding critically ill adults: a clinical practice guideline from the European Society of Intensive Care Medicine.Intensive Care Med. 2020 Apr;46(4):673-696. doi: 10.1007/s00134-019-05884-8. Epub 2020 Jan 7. Intensive Care Med. 2020. PMID: 31912207 Free PMC article.
-
Plasma transfusion in the intensive care unit.Transfusion. 2025 Jan;65(1):73-87. doi: 10.1111/trf.18071. Epub 2024 Dec 18. Transfusion. 2025. PMID: 39696779 Free PMC article.
-
Aggregometry and thromboelastography to identify the timing to trach a COVID-19 patient receiving both antiplatelet therapy and enoxaparin.Clin Case Rep. 2021 Jan 9;9(3):1049-1054. doi: 10.1002/ccr3.3442. eCollection 2021 Mar. Clin Case Rep. 2021. PMID: 33768781 Free PMC article.
-
Prophylactic platelet transfusions prior to surgery for people with a low platelet count.Cochrane Database Syst Rev. 2018 Sep 17;9(9):CD012779. doi: 10.1002/14651858.CD012779.pub2. Cochrane Database Syst Rev. 2018. PMID: 30221749 Free PMC article.
References
-
- Fischler L, Erhart S, Kleger GR, Frutiger A. Prevalence of tracheostomy in ICU patients. A nation-wide survey in Switzerland. Intensive Care Med. 2000;26:1428–33. - PubMed
-
- Esteban A, Anzueto A, Alía I. How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med. 2000;161:1450–8. - PubMed
-
- Heffner JE, Miller KS, Sahn SA. Tracheostomy in the intensive care unit. Part 1: Indications, technique, management. Chest. 1986;90:269–74. - PubMed
-
- Heffner JE, Miller KS, Sahn SA. Tracheostomy in the intensive care unit. Part 2: Complications. Chest. 1986;90:430–6. - PubMed
-
- Sollid SJM, Strand K, Søreide E. Percutanous dilatational tracheotomy in the ICU: a Norwegian survey focusing on perceived risk and safety attitudes. Eur J Anaesthesiol. 2008;25:925–32. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
