

Consideration of the likely benefit from implementation of prostate image-guided radiotherapy using current margin sizes: a radiobiological analysis
- PMID: 22337688
- PMCID: PMC3487058
- DOI: 10.1259/bjr/27924223
Consideration of the likely benefit from implementation of prostate image-guided radiotherapy using current margin sizes: a radiobiological analysis
Abstract
Objective: To estimate the benefit of introduction of image-guided radiotherapy (IGRT) to prostate radiotherapy practice with current clinical target volume-planning target volume (PTV) margins of 5-10 mm.
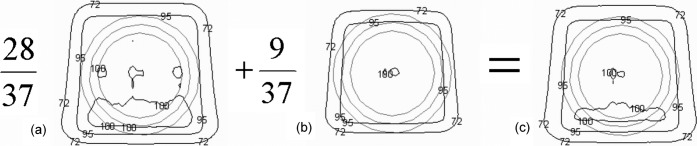
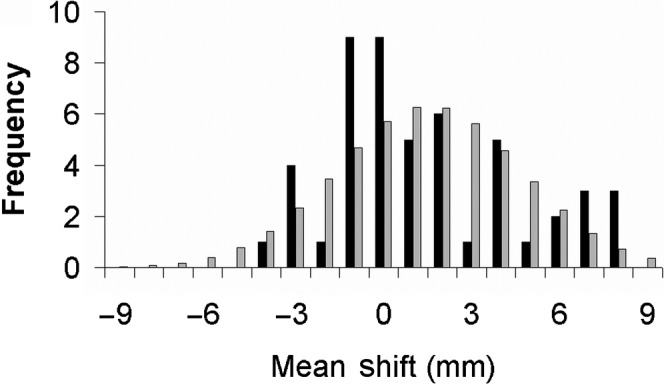
Methods: Systematic error data collected from 50 patients were used together with a random error of σ=3.0 mm to model non-IGRT treatment. IGRT was modelled with residual errors of Σ=σ=1.5 mm. Population tumour control probability (TCP(pop)) was calculated for two three-dimensional conformal radiotherapy techniques: two-phase and concomitant boost. Treatment volumes and dose prescriptions were ostensibly the same. The relative field sizes of the treatment techniques, distribution of systematic errors and correlations between movement axes were examined.
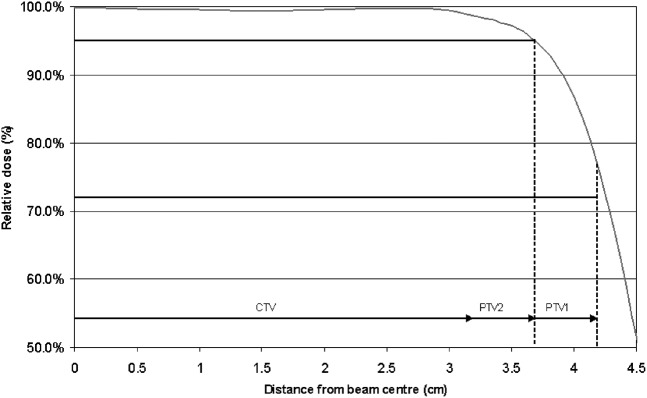
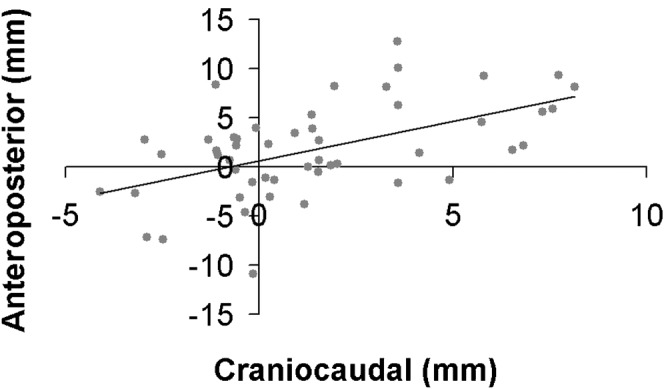
Results: The differences in TCP(pop) between the IGRT and non-IGRT regimes were 0.3% for the two-phase and 1.5% for the concomitant boost techniques. A 2-phase plan, in each phase of which the 95% isodose conformed to its respective PTV, required fields that were 3.5 mm larger than those required for the concomitant boost plan. Despite the larger field sizes, the TCP (without IGRT) in the two-phase plan was only 1.7% higher than the TCP in the concomitant boost plan. The deviation of craniocaudal systematic errors (p=0.02) from a normal distribution, and the correlation of translations in the craniocaudal and anteroposterior directions (p<0.0001) were statistically significant.
Conclusions: The expected population benefit of IGRT for the modelled situation was too small to be detected by a clinical trial of reasonable size, although there was a significant benefit to individual patients. For IGRT to have an observable population benefit, the trial would need to use smaller margins than those used in this study. Concomitant treatment techniques permit smaller fields and tighter conformality than two phases planned separately.
Figures
Similar articles
-
Evaluation of multiple image-based modalities for image-guided radiation therapy (IGRT) of prostate carcinoma: a prospective study.Med Phys. 2013 Apr;40(4):041707. doi: 10.1118/1.4794502. Med Phys. 2013. PMID: 23556877 Clinical Trial.
-
Clinical Implementation of "Plan of the Day" Strategy in Definitive Radiation Therapy of Cervical Cancer: Online Adaptation to Address the Challenge of Organ Filling Reproducibility.Int J Radiat Oncol Biol Phys. 2024 Mar 1;118(3):605-615. doi: 10.1016/j.ijrobp.2023.09.045. Epub 2023 Oct 9. Int J Radiat Oncol Biol Phys. 2024. PMID: 37816473
-
Adaptive image-guided radiotherapy (IGRT) eliminates the risk of biochemical failure caused by the bias of rectal distension in prostate cancer treatment planning: clinical evidence.Int J Radiat Oncol Biol Phys. 2012 Jul 1;83(3):947-52. doi: 10.1016/j.ijrobp.2011.08.025. Epub 2011 Dec 28. Int J Radiat Oncol Biol Phys. 2012. PMID: 22208964
-
Image-guided radiotherapy: a new dimension in radiation oncology.Dtsch Arztebl Int. 2011 Apr;108(16):274-80. doi: 10.3238/arztebl.2011.0274. Epub 2011 Apr 22. Dtsch Arztebl Int. 2011. PMID: 21603562 Free PMC article. Review.
-
A multicentre observational study evaluating image-guided radiotherapy for more accurate partial-breast intensity-modulated radiotherapy: comparison with standard imaging technique.Southampton (UK): NIHR Journals Library; 2014 Nov. Southampton (UK): NIHR Journals Library; 2014 Nov. PMID: 25642565 Free Books & Documents. Review.
Cited by
-
Target margins in radiotherapy of prostate cancer.Br J Radiol. 2016 Nov;89(1067):20160312. doi: 10.1259/bjr.20160312. Epub 2016 Jul 20. Br J Radiol. 2016. PMID: 27377353 Free PMC article. Review.
-
Clinical and radiobiological evaluation of a method for planning target volume generation dependent on organ-at-risk exclusions in magnetic resonance imaging-based prostate radiotherapy.Phys Imaging Radiat Oncol. 2018 Dec 7;8:51-56. doi: 10.1016/j.phro.2018.11.007. eCollection 2018 Oct. Phys Imaging Radiat Oncol. 2018. PMID: 33458417 Free PMC article.
-
Image-guided radiotherapy of the prostate using daily CBCT: the feasibility and likely benefit of implementing a margin reduction.Br J Radiol. 2014 Dec;87(1044):20140459. doi: 10.1259/bjr.20140459. Epub 2014 Oct 29. Br J Radiol. 2014. PMID: 25354015 Free PMC article. Clinical Trial.
References
-
- van Herk M. Errors and margins in radiotherapy. Semin Radiat Oncol 2004;14:52–64 - PubMed
-
- Schallenkamp J, Herman M, Kruse J, Pisansky T. Prostate position relative to pelvic bony anatomy based on intraprostatic gold markers and electronic portal imaging. Int J Radiat Oncol Biol Phys 2005;63:800–11 - PubMed
-
- Burnet NG, Adams EJ, Fairfoul J, Tudor GS, Hoole AC, Routsis DS, et al. Practical aspects of implementation of helical tomotherapy for intensity-modulated and image-guided radiotherapy. Clin Oncol 2010;22:294–312 - PubMed
-
- Broggi S, Cozzarini C, Fiorino C, Maggiulli E, Alongi F, Cattaneo GM, et al. Modeling set-up error by daily MVCT for prostate adjuvant treatment delivered in 20 fractions: implications for the assessment of the optimal correction strategies. Radiother Oncol 2009;93:246–52 - PubMed
-
- Herman MG, Pisansky TM, Kruse JJ, Prisciandaro JI, Davis BJ, King BF. Technical aspects of daily online positioning of the prostate for three-dimensional conformal radiotherapy using an electronic portal imaging device. Int J Radiat Oncol Biol Phys 2003;57:1131–40 - PubMed
