

Catheter-deliverable hydrogel derived from decellularized ventricular extracellular matrix increases endogenous cardiomyocytes and preserves cardiac function post-myocardial infarction
- PMID: 22340268
- PMCID: PMC3285410
- DOI: 10.1016/j.jacc.2011.10.888
Catheter-deliverable hydrogel derived from decellularized ventricular extracellular matrix increases endogenous cardiomyocytes and preserves cardiac function post-myocardial infarction
Abstract
Objectives: This study evaluated the use of an injectable hydrogel derived from ventricular extracellular matrix (ECM) for treating myocardial infarction (MI) and its ability to be delivered percutaneously.
Background: Injectable materials offer promising alternatives to treat MI. Although most of the examined materials have shown preserved or improved cardiac function in small animal models, none have been specifically designed for the heart, and few have translated to catheter delivery in large animal models.
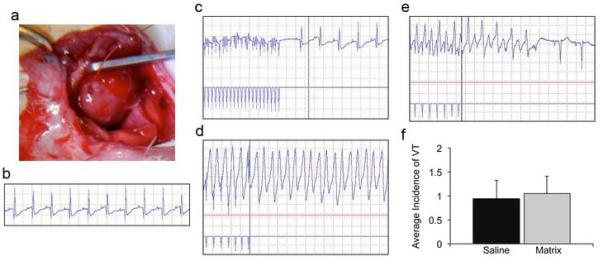
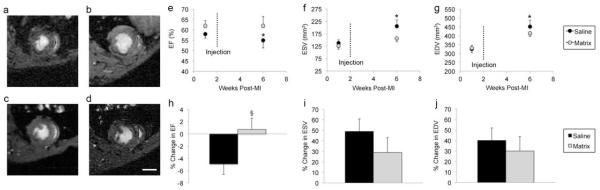
Methods: We have developed a myocardial-specific hydrogel, derived from decellularized ventricular ECM, which self-assembles when injected in vivo. Female Sprague-Dawley rats underwent ischemia reperfusion followed by injection of the hydrogel or saline 2 weeks later. The implantation response was assessed via histology and immunohistochemistry, and the potential for arrhythmogenesis was examined using programmed electrical stimulation 1 week post-injection. Cardiac function was analyzed with magnetic resonance imaging 1 week pre-injection and 4 weeks post-MI. In a porcine model, we delivered the hydrogel using the NOGA-guided MyoStar catheter (Biologics Delivery Systems, Irwindale, California), and utilized histology to assess retention of the material.
Results: We demonstrate that injection of the material in the rat MI model increases endogenous cardiomyocytes in the infarct area and maintains cardiac function without inducing arrhythmias. Furthermore, we demonstrate feasibility of transendocardial catheter injection in a porcine model.
Conclusions: To our knowledge, this is the first in situ gelling material to be delivered via transendocardial injection in a large animal model, a critical step towards the translation of injectable materials for treating MI in humans. Our results warrant further study of this material in a large animal model of MI and suggest this may be a promising new therapy for treating MI.
© 2012 American College of Cardiology Foundation.
Figures



References
-
- Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics -- 2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:480–6. - PubMed
-
- Mann DL. Mechanisms and models in heart failure: A combinatorial approach. Circulation. 1999;100:999–1008. - PubMed
-
- Smits PC, van Geuns RJ, Poldermans D, et al. Catheter-based intramyocardial injection of autologous skeletal myoblasts as a primary treatment of ischemic heart failure: clinical experience with six-month follow-up. J Am Coll Cardiol. 2003;42:2063–9. - PubMed
-
- Dib N, Diethrich EB, Campbell A, et al. Endoventricular transplantation of allogenic skeletal myoblasts in a porcine model of myocardial infarction. J Endovasc Ther. 2002;9:313–9. - PubMed
-
- Dib N, Campbell A, Jacoby DB, et al. Safety and feasibility of percutaneous autologous skeletal myoblast transplantation in the coil-infarcted swine myocardium. J Pharmacol Toxicol Methods. 2006;54:71–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
