

Cerebral microinfarcts: the invisible lesions
- PMID: 22341035
- PMCID: PMC3359329
- DOI: 10.1016/S1474-4422(11)70307-6
Cerebral microinfarcts: the invisible lesions
Abstract
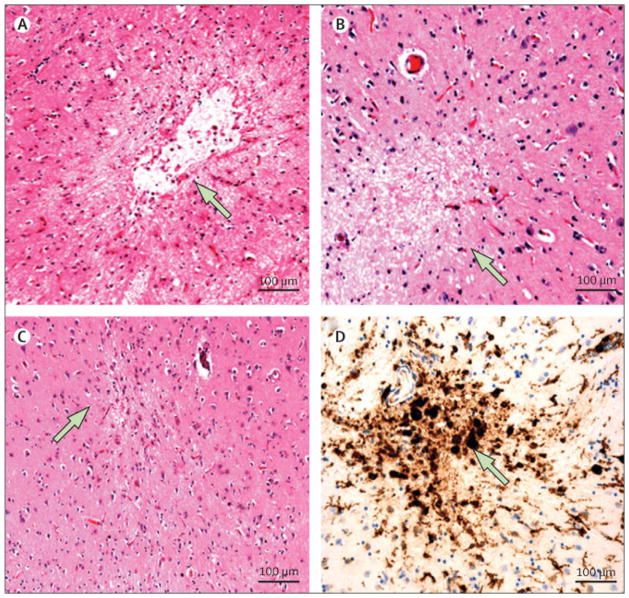
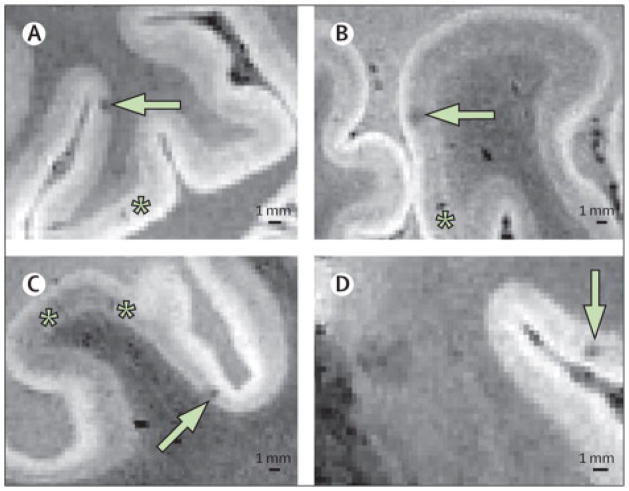
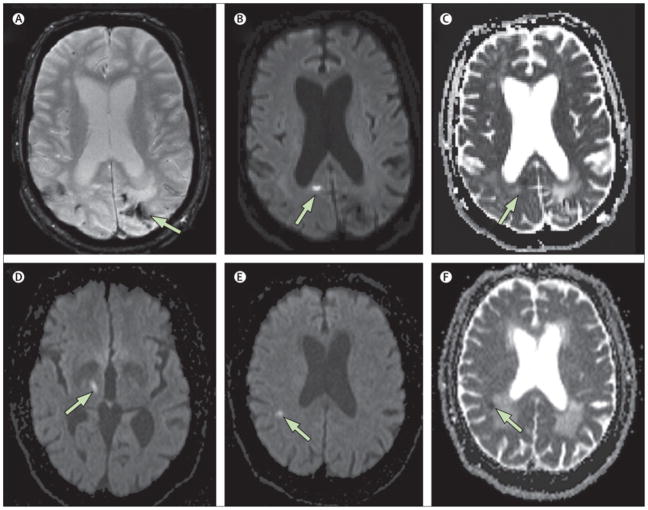
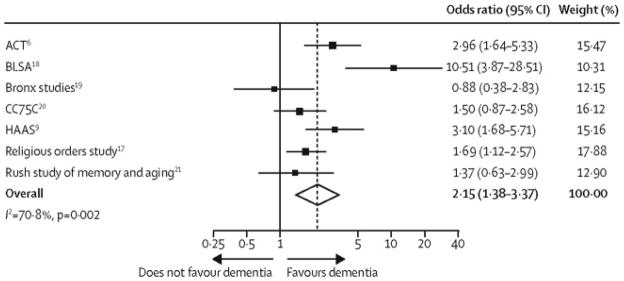
The association between small but still visible lacunar infarcts and cognitive decline has been established by population-based radiological and pathological studies. Microscopic examination of brain sections shows even smaller but substantially more numerous microinfarcts, the focus of this Review. These lesions often result from small vessel pathologies such as arteriolosclerosis or cerebral amyloid angiopathy. They typically go undetected in clinical-radiological correlation studies that rely on conventional structural MRI, although the largest acute microinfarcts can be detected by diffusion-weighted imaging. In view of their high numbers and widespread distribution, microinfarcts could directly disrupt important cognitive networks and thus account for some of the neurological dysfunction associated with lesions visible on conventional MRI such as lacunar infarcts and white matter hyperintensities. Standardised neuropathological assessment criteria and the development of non-invasive means of detection during life would be major steps towards understanding the causes and consequences of otherwise macroscopically invisible microinfarcts.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Dr. Smith reports no conflicts of interest. Dr. Schneider reports serving as a consultant to AVID Radiopharmaceuticals, and serving on advisory boards to Eli Lilly and Company and GE Healthcare. Dr. Wardlaw reports no conflicts of interest. Dr. Greenberg reports no conflicts of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
