

Evaluation of GI bleeding after implantation of left ventricular assist device
- PMID: 22341716
- PMCID: PMC3835739
- DOI: 10.1016/j.gie.2011.12.014
Evaluation of GI bleeding after implantation of left ventricular assist device
Abstract
Background: Left ventricular assist devices (LVADs) have revolutionized the management of end-stage heart failure (ESHF). However, unexpectedly high rates of GI bleeding (GIB) have been described, and etiology and outcome remain unclear.
Objective: To determine the prevalence, etiology, and outcome of GIB in LVAD recipients.
Design: Retrospective case series.
Setting: Tertiary care academic university hospital.
Patients: 154 ESHF patients (55.4 years, 122 men/32 women) with LVADs implanted over a 10-year period.
Main outcome measurements: Overt or occult GIB prompting endoscopic evaluation ≥ 7 days after LVAD implantation.
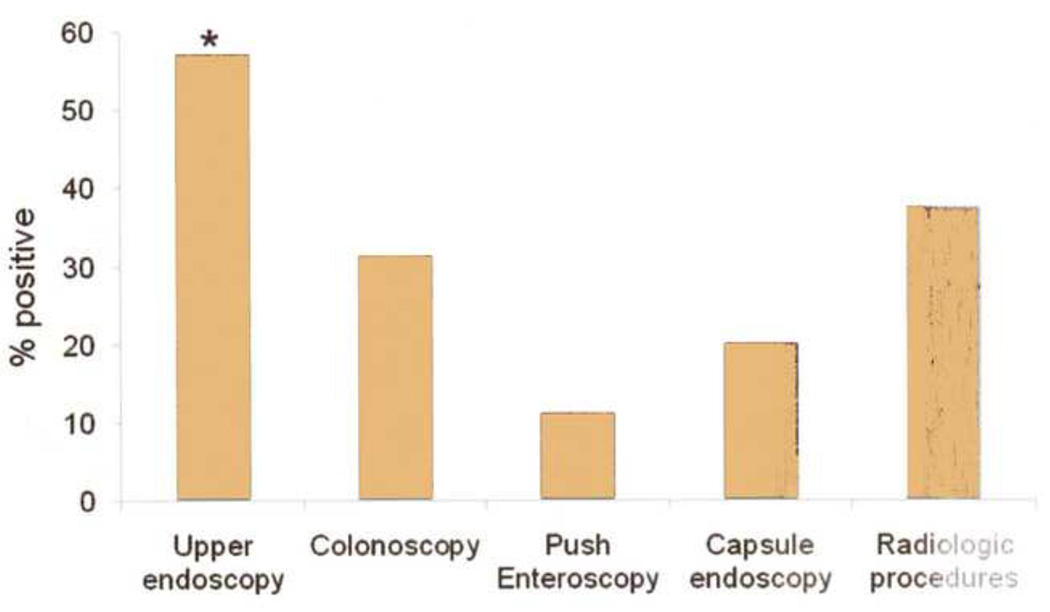
Results: Over a mean of 0.9 ± 0.1 years of follow-up, 29 patients (19%) experienced 44 GIB episodes. Patients with GIB were older and received anticoagulation therapy before devices were implanted (P ≤ .02 for each). GIB was overt (n = 31) rather than occult (n = 13), and most patients presented with melena (n = 22, 50%); hemodynamic instability was observed in 13.6%. Each bleeding episode required 2.1 ± 0.1 diagnostic or therapeutic procedures, and a source was localized in 71%. Upper endoscopy provided the highest diagnostic yield; peptic bleeding (n = 14) and vascular malformations (n = 8) dominated the findings. Endoscopy was safe and well tolerated. Overall mortality was 35%, none directly from GIB.
Limitation: Retrospective design.
Conclusions: Rates of GIB with LVADs are higher than that seen in other patient populations, including those receiving anticoagulation and antiplatelet therapy. GIB episodes are mostly overt and predominantly from the upper GI tract. Endoscopy is safe in the LVAD population.
Copyright © 2012 American Society for Gastrointestinal Endoscopy. Published by Mosby, Inc. All rights reserved.
Figures
Similar articles
-
Timing of Gastrointestinal Bleeding After Implantation of Left Ventricular Assist Devices Associates With Anatomic Location, Presentation, and Management.Clin Gastroenterol Hepatol. 2019 Feb;17(3):448-454. doi: 10.1016/j.cgh.2018.05.056. Epub 2018 Jun 12. Clin Gastroenterol Hepatol. 2019. PMID: 29906524
-
A Multicenter Study of Left Ventricular Assist Device-Related Gastrointestinal Bleeding.Clin Transl Gastroenterol. 2022 Oct 1;13(10):e00526. doi: 10.14309/ctg.0000000000000526. Clin Transl Gastroenterol. 2022. PMID: 36007177 Free PMC article.
-
Limited usefulness of endoscopic evaluation in patients with continuous-flow left ventricular assist devices and gastrointestinal bleeding.J Heart Lung Transplant. 2018 Jun;37(6):723-732. doi: 10.1016/j.healun.2017.12.017. Epub 2017 Dec 20. J Heart Lung Transplant. 2018. PMID: 29402604
-
Left ventricular assist devices and gastrointestinal bleeding: a narrative review of case reports and case series.Clin Cardiol. 2013 Apr;36(4):190-200. doi: 10.1002/clc.22096. Epub 2013 Feb 3. Clin Cardiol. 2013. PMID: 23378047 Free PMC article. Review.
-
Gastrointestinal Bleeding in Patients Supported with Left Ventricular Assist Devices: The Journey from Bridging to Destination.Am J Cardiol. 2023 Aug 15;201:71-77. doi: 10.1016/j.amjcard.2023.05.059. Epub 2023 Jun 21. Am J Cardiol. 2023. PMID: 37352668 Review.
Cited by
-
A population based analysis of trends, risk factors and outcomes associated with gastrointestinal bleeding in patients with left ventricular assist devices.Am J Cardiovasc Dis. 2020 Aug 15;10(3):247-257. eCollection 2020. Am J Cardiovasc Dis. 2020. PMID: 32923107 Free PMC article.
-
Gastrointestinal angiodysplasia is associated with significant gastrointestinal bleeding in patients with continuous left ventricular assist devices.Endosc Int Open. 2016 Mar;4(3):E371-7. doi: 10.1055/s-0042-101752. Endosc Int Open. 2016. PMID: 27004257 Free PMC article.
-
Patient management important for long-term support beyond 5 years in the BTT: republication of the article published in the Japanese Journal of Artificial Organs.J Artif Organs. 2024 Sep;27(3):182-187. doi: 10.1007/s10047-024-01441-3. Epub 2024 Mar 29. J Artif Organs. 2024. PMID: 38548928 Review.
-
Safety and efficacy of single-balloon enteroscopy in management of gastrointestinal bleeding in patients with a left ventricular assist device.Endosc Int Open. 2017 Mar;5(3):E179-E183. doi: 10.1055/s-0043-102397. Endosc Int Open. 2017. PMID: 28299353 Free PMC article.
-
Relationship Between Anticoagulation Intensity and Thrombotic or Bleeding Outcomes Among Outpatients With Continuous-Flow Left Ventricular Assist Devices.Circ Heart Fail. 2016 May;9(5):e002680. doi: 10.1161/CIRCHEARTFAILURE.115.002680. Circ Heart Fail. 2016. PMID: 27154497 Free PMC article.
References
-
- McMurray JJ. Clinical practice. Systolic heart failure. N Engl J Med. 2010;362(3):228–238. - PubMed
-
- Johnson MR, Meyer KH, Haft J, Kinder D, Webber SA, Dyke DB. Heart transplantation in the United States, 1999–2008. Am J Transplant. 2010;10(4 Pt 2):1035–1046. - PubMed
-
- Rose EA, Gelijns AC, Moskowitz AJ, Heitjan DF, Stevenson LW, Dembitsky W, et al. Long-term use of a left ventricular assist device for end-stage heart failure. N Engl J Med. 2001;345(20):1435–1443. - PubMed
-
- Miller LW, Pagani FD, Russell SD, John R, Boyle AJ, Aaronson KD, et al. Use of a continuous-flow device in patients awaiting heart transplantation. N Engl J Med. 2007;357(9):885–896. - PubMed
-
- Slaughter MS, Rogers JG, Milano CA, Russell SD, Conte JV, Feldman D, et al. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med. 2009;361(23):2241–2251. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
