

Risk factors for unintended durotomy during spine surgery: a multivariate analysis
- PMID: 22342249
- PMCID: PMC3299921
- DOI: 10.1016/j.spinee.2012.01.012
Risk factors for unintended durotomy during spine surgery: a multivariate analysis
Abstract
Background context: Incidental durotomy during spine surgery is a common occurrence, with a reported incidence ranging from 3% to 16%. Risk factors identified by prior studies include age, type of procedure, revision surgery, ossification of the posterior longitudinal ligament, gender, osteoporosis, and arthritis. However, these studies are largely univariate analyses using retrospectively recorded data.
Purpose: To identify and quantify statistically significant risk factors for inadvertent durotomy during spine surgery.
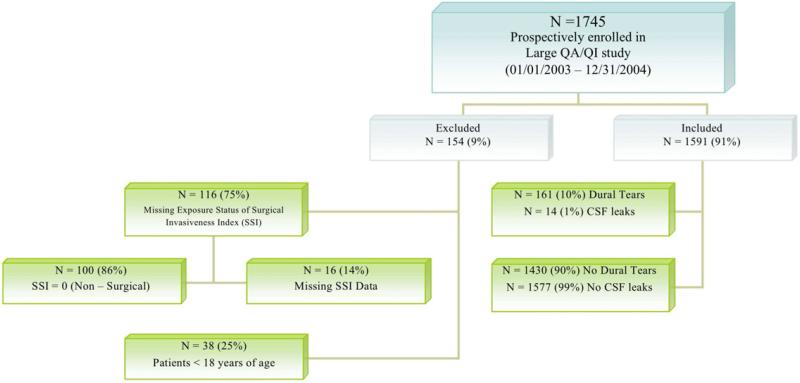
Study design: Multivariate analysis of prospectively collected registry data. The University of Washington Spine End Results Registry 2003 and 2004 is a compilation of prospectively collected detailed data on 1,745 patients who underwent spine surgery during 2003 to 2004.
Patient sample: One thousand seven hundred forty-five patients underwent spine surgery from 2003 to 2004 at our two institutions.
Outcome measures: Cardiac, pulmonary, gastrointestinal, neurologic, renal, and urologic complications defined a priori data collection.
Methods: Using these data, univariate and multivariate statistical analyses were performed to identify and quantify risk factors for incidental durotomy during spine surgery. Relative risk (RR) values with valid confidence intervals and p values were determined using these data.
Results: Our multivariate analysis demonstrated that age, lumbar surgery, revision surgery, and elevated surgical invasiveness are significant risk factors for unintended durotomy. Of these, revision surgery was the strongest risk factor for dural tear (RR, 2.21). Diabetes was a significant risk factor in the univariate analysis but not in the multivariate analysis.
Conclusions: Revision surgery, age, lumbar surgery, degenerative disease, and elevated surgical invasiveness are significant risk factors for unintended durotomy during spine surgery. These data can be useful to surgeons and patients when considering surgical treatment.
Copyright © 2012 Elsevier Inc. All rights reserved.
References
-
- Khan MH, et al. Postoperative management protocol for incidental dural tears during degenerative lumbar spine surgery: a review of 3,183 consecutive degenerative lumbar cases. Spine (Phila Pa 1976) 2006;31(22):2609–13. - PubMed
-
- Sin AH, et al. Predictive factors for dural tear and cerebrospinal fluid leakage in patients undergoing lumbar surgery. J Neurosurg Spine. 2006;5(3):224–7. - PubMed
-
- Wang JC, Bohlman HH, Riew KD. Dural tears secondary to operations on the lumbar spine. Management and results after a two-year-minimum follow-up of eighty-eight patients. J Bone Joint Surg Am. 1998;80(12):1728–32. - PubMed
-
- Cammisa FP, Jr., et al. Incidental durotomy in spine surgery. Spine (Phila Pa 1976) 2000;25(20):2663–7. - PubMed
-
- Brookfield K, et al. Delayed symptoms of cerebrospinal fluid leak following lumbar decompression. Orthopedics. 2008;31(8):816. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
