

A cluster randomized trial of an enhanced eGFR prompt in chronic kidney disease
- PMID: 22344504
- PMCID: PMC3315340
- DOI: 10.2215/CJN.12391211
A cluster randomized trial of an enhanced eGFR prompt in chronic kidney disease
Abstract
Background and objectives: Despite reporting estimated GFR (eGFR), use of evidence-based interventions in CKD remains suboptimal. This study sought to determine the effect of an enhanced eGFR laboratory prompt containing specific management recommendations, compared with standard eGFR reporting in CKD.
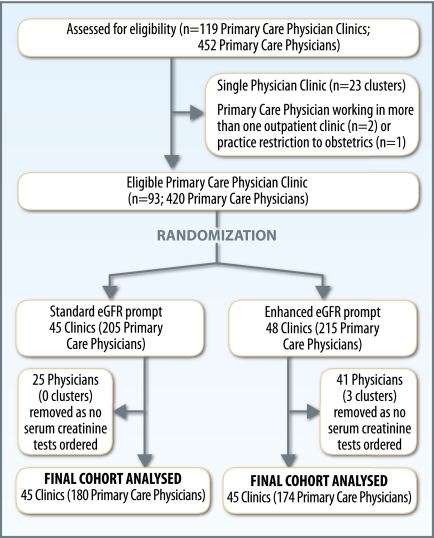
Design, setting, participants, & measurements: A cluster randomized trial of a standard or enhanced eGFR laboratory prompt was performed in 93 primary care practices in Alberta, Canada. Although all adult patients with CKD (eGFR <60 ml/min per 1.73 m(2)) were included, medication data were only available for elderly patients (aged ≥66 years). The primary outcome, the proportion of patients with diabetes or proteinuria receiving an angiotensin converting enzyme inhibitor (ACEi) or angiotensin receptor blocker (ARB), was assessed in elderly CKD patients.
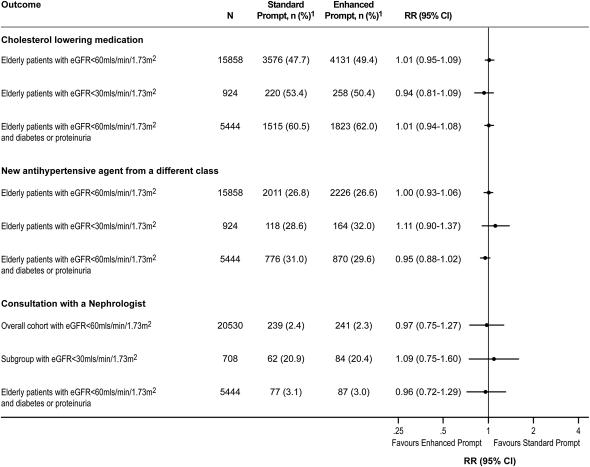
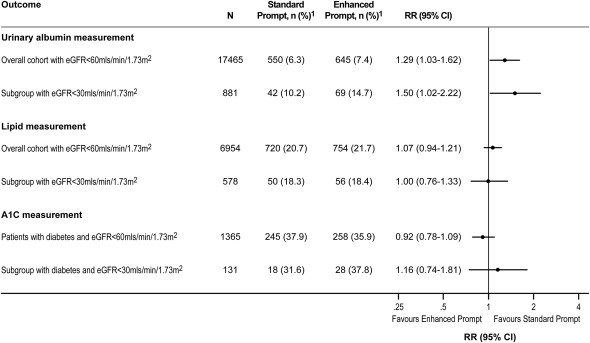
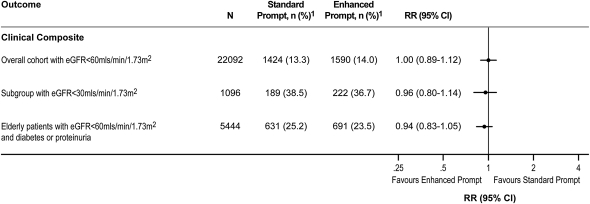
Results: There were 5444 elderly CKD patients with diabetes or proteinuria who were eligible for primary outcome assessment, irrespective of baseline ACEi/ARB use. ACEi/ARB use in the subsequent year was 77.1% and 76.9% in the standard and enhanced prompt groups, respectively. In the subgroup of elderly patients with an eGFR <30 ml/min per 1.73 m(2), ACEi/ARB use was higher in the enhanced prompt group. Among 22,092 CKD patients, there was no difference in the likelihood of a composite clinical outcome (death, ESRD, doubling of serum creatinine, or hospitalization for myocardial infarction, heart failure, or stroke) over a median of 2.1 years.
Conclusions: In elderly patients with CKD and an indication for ACEi/ARB, an enhanced laboratory prompt did not increase use of these medications.
Figures
Comment in
-
Decision support and CKD: not there yet.Clin J Am Soc Nephrol. 2012 Apr;7(4):525-6. doi: 10.2215/CJN.02140212. Epub 2012 Mar 15. Clin J Am Soc Nephrol. 2012. PMID: 22422537 No abstract available.
References
-
- National Kidney Foundation : K/DOQI clinical practice guidelines for chronic kidney disease: Evaluation, classification, and stratification. Am J Kidney Dis 39[Suppl 1]: S1–S266, 2002 - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- James MT, Hemmelgarn BR, Wiebe N, Pannu N, Manns BJ, Klarenbach SW, Tonelli M, Alberta Kidney Disease Network : Glomerular filtration rate, proteinuria, and the incidence and consequences of acute kidney injury: A cohort study. Lancet 376: 2096–2103, 2010 - PubMed
-
- Hemmelgarn BR, Manns BJ, Lloyd A, James MT, Klarenbach S, Quinn RR, Wiebe N, Tonelli M, Alberta Kidney Disease Network : Relation between kidney function, proteinuria, and adverse outcomes. JAMA 303: 423–429, 2010 - PubMed
-
- Tonelli M, Bohm C, Pandeya S, Gill J, Levin A, Kiberd BA: Cardiac risk factors and the use of cardioprotective medications in patients with chronic renal insufficiency. Am J Kidney Dis 37: 484–489, 2001 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
