

Use of secondary prevention medications among adults with reduced kidney function
- PMID: 22344513
- PMCID: PMC3315345
- DOI: 10.2215/CJN.11441111
Use of secondary prevention medications among adults with reduced kidney function
Abstract
Background and objectives: Persons with kidney disease often have cardiovascular disease, but they are less likely to use recommended medications for secondary prevention. The hypothesis was that participants with reduced estimated GFR have lower use of medications recommended for secondary prevention of cardiovascular events (antiplatelet agents, angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, β-blockers, and statins) and lower medication adherence than participants with preserved estimated GFR.
Design, setting, participants, & measurements: In this cross-sectional analysis, we analyzed data from 6913 participants in the Reasons for Geographic and Racial Differences in Stroke study with a history of cardiovascular disease. Medication use was ascertained by an in-home pill bottle review. Medication adherence was assessed using a validated four-item scale.
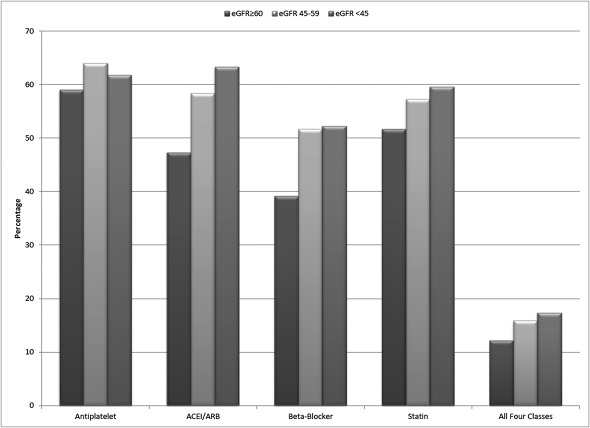
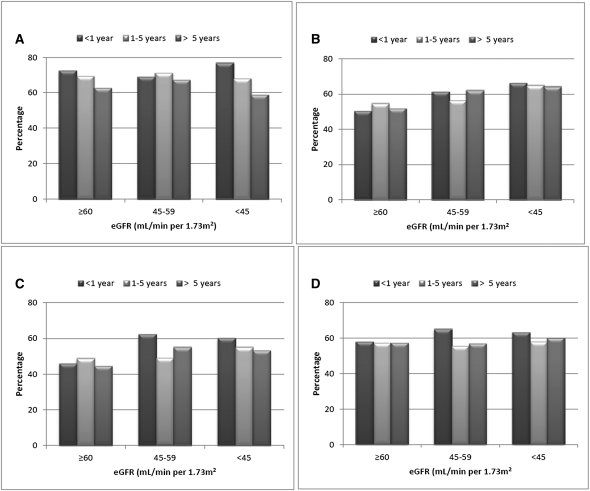
Results: Among participants with a history of cardiovascular disease, 59.8% used antiplatelet agents, 49.9% used angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, 41.6% used β-blockers, and 53.0% used statins. Compared with the referent group (estimated GFR ≥60 ml/min per 1.73 m(2)), participants with estimated GFR <45 ml/min per 1.73 m(2) were more likely to use angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers (adjusted prevalence ratio=1.14, 95% confidence interval=1.06-1.23), β-blockers (adjusted prevalence ratio=1.20, 95% confidence interval=1.09-1.32), and statins (adjusted prevalence ratio=1.10, 95% confidence interval=1.01-1.19). Antiplatelet agent use did not differ by estimated GFR category; 30% of participants reported medication nonadherence across all categories of estimated GFR.
Conclusions: Among participants with a history of cardiovascular disease, mild to moderate reductions in estimated GFR were associated with similar and even more frequent use of medications for secondary prevention compared with participants with preserved estimated GFR. Overall medication use and adherence were suboptimal.
Figures
References
-
- National Kidney Foundation: KDOQI Clinical Practice Guidelines on Hypertension and Antihypertensive Agents in Chronic Kidney Disease, 2002. Available at http://www.kidney.org/professionals/KDOQI/guidelines_bp/index.htm Accessed May 25, 2010 - PubMed
-
- McClellan WM, Langston RD, Presley R: Medicare patients with cardiovascular disease have a high prevalence of chronic kidney disease and a high rate of progression to end-stage renal disease. J Am Soc Nephrol 15: 1912–1919, 2004 - PubMed
-
- Smith SC, Jr, Allen J, Blair SN, Bonow RO, Brass LM, Fonarow GC, Grundy SM, Hiratzka L, Jones D, Krumholz HM, Mosca L, Pasternak RC, Pearson T, Pfeffer MA, Taubert KA, AHA/ACC. National Heart, Lung, and Blood Institute : AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update: Endorsed by the National Heart, Lung, and Blood Institute. Circulation 113: 2363–2372, 2006 - PubMed
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
