

Patients with a history of infection and voiding dysfunction are at risk for recurrence after successful endoscopic treatment of vesico ureteral reflux and deserve long-term follow up
- PMID: 22346096
- PMCID: PMC3271445
- DOI: 10.4103/0974-7796.91616
Patients with a history of infection and voiding dysfunction are at risk for recurrence after successful endoscopic treatment of vesico ureteral reflux and deserve long-term follow up
Abstract
Aim of the study: Subureteral endoscopic injection of a bulking agent is an attractive alternative to open surgery or antibiotic prophylaxis for vesico ureteral reflux (VUR). Little information is available about long-term risk of recurrence after an initially successful treatment. Aim of this paper was to review short- and long-term success rate of endoscopic treatment in a single Center series after risk stratification of individual patients.
Materials and methods: The records of 126 patients who underwent Deflux injection for primary VUR were examined. Indications to treatment were an unvaried high grade VUR (IV-V) at 1 year from diagnosis and/or and recurrent urinary tract infection (UTI) on antibiotic prophylaxis even in the presence of mild grade VUR (III grade). Gender, age and mode of diagnosis, infections (UTI), voiding dysfunctions, VUR grade and side, renal function, number of treatments were correlated to outcome. Long-term evaluation was planned at a minimum of 1 year from the last negative post-injection cystogram (MCUG). A new MCUG and DMSA scan were also offered to those complaining new UTI episodes. Late recurrences were correlated to history and grade of reflux. Data were analyzed with Graph Pad Instat software; the Chi-square test was used for univariate comparisons, the Fisher's exact test for categorical variables.and multiple regression tests for factors influencing outcome.
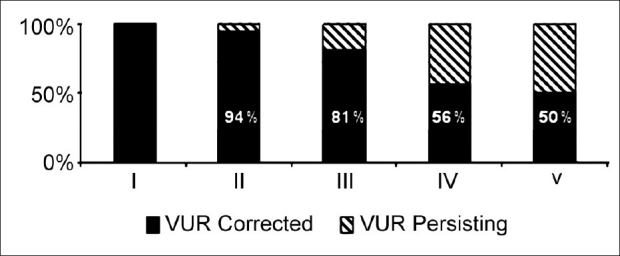
Results: M/F ratio was 62 to 64; median age at diagnosis was 28 months. VUR affected 198 renal units. Preinjection VUR grade was I in 1, II in 27, III in 107, IV in 59, and V in 4 units. Reduced DMSA uptake was evidenced in 51 units and scarring in 24. Median age at treatment was 34.5 months, for persistent high grade VUR (IV-V) in 55 patients and recurrent IVU in 92. Two hundred sixty seven injections were performed on 198 ureters. Complete resolution was documented by MCUG at 3-5 months in 68%, low grading < II in 20%, persistence or unsignificant reduction in 11%. Preoperative recurrent UTI, higher grade VUR, and bilaterality were correlated to a poorer surgical outcome. Among 80 successfully treated cases, 12 complained of persistent UTI. Recurrence of VUR was demonstrated in 31% of them. Deteriorated uptake or additional scarring in 25% was independent from VUR recurrence. Preoperative recurrent UTI and voiding dysfunction correlated significantly to late outcome.
Conclusions: Preoperative recurrent IVU, together with high-grade reflux, seem to correlate to lower success rate of Deflux injection for primary VUR. Even after successful endoscopic treatment, long-term surveillance may be needed among these cases, mainly if voiding dysfunction is also recorded. Late recurring VUR must be actively excluded in case of new IVU episodes.
Keywords: Endoscopic treatment; urinary tract infection; vesico ureteral reflux.
Conflict of interest statement
Figures
Similar articles
-
Vesicoureteral Reflux.2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 33085409 Free Books & Documents.
-
[Vesicoureteral reflux grades III-IV: factors involved in the efficacy of endoscopic treatment in pediatric patients].Arch Esp Urol. 2006 Mar;59(2):155-67. doi: 10.4321/s0004-06142006000200006. Arch Esp Urol. 2006. PMID: 16649521 Spanish.
-
Factors affecting the success of endoscopic treatment of vesicoureteral reflux and comparison of two dextranomer based bulking agents: does bulking substance matter?J Pediatr Urol. 2015 Apr;11(2):90.e1-5. doi: 10.1016/j.jpurol.2014.12.009. Epub 2015 Mar 2. J Pediatr Urol. 2015. PMID: 25791422
-
Controversies Regarding Management of Vesico-ureteric Reflux.Indian J Pediatr. 2017 Jul;84(7):540-544. doi: 10.1007/s12098-017-2359-4. Epub 2017 May 6. Indian J Pediatr. 2017. PMID: 28477320 Review.
-
Surgical management of vesicoureteral reflux in children.Pediatr Nephrol. 2012 Apr;27(4):551-61. doi: 10.1007/s00467-011-1933-7. Epub 2011 Jun 22. Pediatr Nephrol. 2012. PMID: 21695451 Free PMC article. Review.
Cited by
-
Local tissue reaction and histopathological characteristics of three different bulking agents: a rabbit model.Int Braz J Urol. 2021 Mar-Apr;47(2):322-332. doi: 10.1590/S1677-5538.IBJU.2020.0171. Int Braz J Urol. 2021. PMID: 33146977 Free PMC article.
-
Predictors of reflux persistence after endoscopic dextranomer/hyaluronic Acid copolymer injection in pediatric patients with Vesicoureteral reflux: short-term results.Sci Rep. 2024 Jul 2;14(1):15252. doi: 10.1038/s41598-024-62449-6. Sci Rep. 2024. PMID: 38956126 Free PMC article.
References
-
- Decter RM. Vescicoureteral reflux. Pediatr Rev. 2001;22:205–10. - PubMed
-
- Hellerstein S. Recurrent urinary tract infections in children. Pediatr Infect Dis. 1982;1:271–81. - PubMed
-
- Layton KL. Diagnosis and management of pediatric urinary tract infections. Clin Fam Pract. 2003;165:23–8.
-
- Capozza N, Lais A, Matarazzo E, Nappo S, Patricolo M, Caione P. Treatment of vesico-ureteric reflux: A new algorithm based on parental preference. BJU Int. 2003;92:285–8. - PubMed
-
- Rushton HG, Majd M, Jantausch B, Wiedermann BL, Belman AB. Renal scarring following reflux and nonreflux pyelonephritis in children: Evaluation with 99mtechnetium-dimercaptosuccinic acid scintigraphy. J Urol. 1992;147:1327–32. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
