

Long term therapy of cytomegalovirus retinitis with ganciclovir in a child with acquired immunodeficiency syndrome
- PMID: 22346413
- PMCID: PMC3250807
- DOI: 10.1155/1993/576891
Long term therapy of cytomegalovirus retinitis with ganciclovir in a child with acquired immunodeficiency syndrome
Abstract
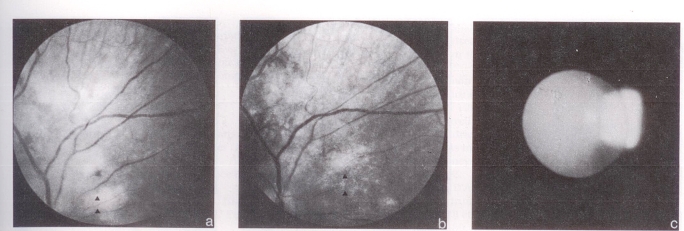
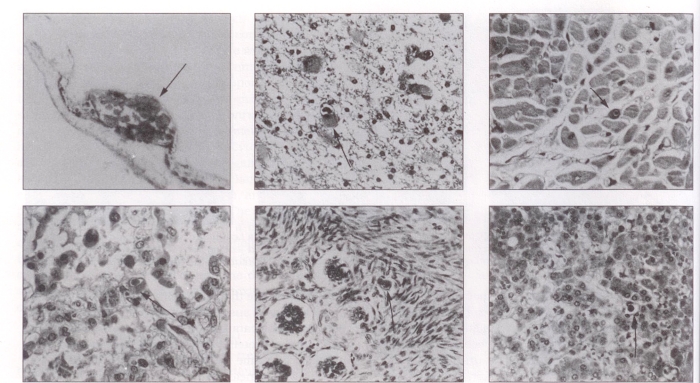
Cytomegalovirus retinitis is the most severe ophthalmological complication of patients with acquired immune deficiency syndrome (aids). Ganciclovir must be given continuously to control progression of the disease or relapse typically occurs. Data in children are limited; this report describes a nine-year-old boy with transfusion-acquired aids who was treated with ganciclovir for 23 months for control of cytomegalovirus retinitis. The retinal disease was exacerbated when ganciclovir was temporarily withheld because of presumed drug toxicity, and improved with re-institution of therapy. When ganciclovir was finally discontinued because of complete loss of vision, the patient rapidly deteriorated and died; widespread cytomegalovirus infection was found at autopsy. Subcapsular cataracts appearing during therapy were thought to be a toxic effect of ganciclovir. Ganciclovir can be effective in controlling cytomegalovirus retinitis in children; however, similarities in laboratory findings may lead to confusion between systemic drug toxicity and disease progression.
La rétinite à cytomégalovirus (CMV) est la complication ophtalmologique la plus grave qui puisse survenir chez les sidatiques. L’administration continue de ganciclovir est indispensable pour contrôler l’évolution de la maladie, sans quoi les rechutes surviennent typiquement. Les données relatives aux enfants sont limitées. Le présent rapport décrit le cas d’un garçon âgé de neuf ans, ayant contracté le SIDA à la suite d’une transfusion sanguine, et qui a été traité par le ganciclovir pendant 23 mois pour contrôler une rétinite à cytomégalovirus. La maladie a été exacerbée par l’arrêt temporaire du médicament, motivé par sa présumée toxicité, et améliorée dès la reprise du traitement. Quand la thérapie a été définitivement interrompue en raison d’une cécité totale, l’état du patient s’est rapidement détérioré et il est décédé. L’étendue de l’infection à CMV a été constatée à l’autopsie. Les cataractes sous-capsulaires apparues au cours du traitement sont attribuées à l’effet toxique du ganciclovir. Le médicament peut contrôler efficacement la rétinite à CMV chez l’enfant. Cependant, la similarité des résultats de laboratoire peut créer une confusion entre une toxicité médicamenteuse systémique et l’évolution de la maladie.
Keywords: Acquired immune deficiency syndrome (AIDS); Cataracts; Cytomegalovirus; Ganciclovir; Retinitis.
Figures
Similar articles
-
AIDS-CMV retinitis: Singapore's first cases.Ann Acad Med Singap. 1990 Nov;19(6):781-7. Ann Acad Med Singap. 1990. PMID: 1966662
-
Serious cytomegalovirus disease in the acquired immunodeficiency syndrome (AIDS). Clinical findings, diagnosis, and treatment.Ann Intern Med. 1988 Apr;108(4):585-94. doi: 10.7326/0003-4819-108-4-585. Ann Intern Med. 1988. PMID: 2831765 Review.
-
Cytomegalovirus retinitis and acquired immunodeficiency syndrome.Arch Ophthalmol. 1989 Jan;107(1):75-80. doi: 10.1001/archopht.1989.01070010077031. Arch Ophthalmol. 1989. PMID: 2535932
-
Combination foscarnet and ganciclovir therapy vs monotherapy for the treatment of relapsed cytomegalovirus retinitis in patients with AIDS. The Cytomegalovirus Retreatment Trial. The Studies of Ocular Complications of AIDS Research Group in Collaboration with the AIDS Clinical Trials Group.Arch Ophthalmol. 1996 Jan;114(1):23-33. doi: 10.1001/archopht.1996.01100130021004. Arch Ophthalmol. 1996. PMID: 8540847 Clinical Trial.
-
Ocular complications of the acquired immunodeficiency syndrome. Focus on the treatment of cytomegalovirus retinitis with ganciclovir and foscarnet.Pharm World Sci. 1993 Apr 23;15(2):56-67. doi: 10.1007/BF01874084. Pharm World Sci. 1993. PMID: 8387852 Review.
References
-
- Oxtoby MJ. Perinatally acquired human immunodeficiency virus infection. Pediatr Infect Dis J. 1990;9:609–19. - PubMed
-
- Federal Centre for aids aids surveillance in Canada. CDWR. 1990;16:93–5.
-
- Falloon J, Eddy J, Wiener L, Pizzo PA. Human immunodeficiency virus infection in children. J Pediatr. 1989;114:1–30. - PubMed
-
- Schooley RT. Cytomegalovirus in the setting of infection with human immunodeficiency virus. Rev Infect Dis. 1990;12:S811–9. - PubMed
-
- Frenkel LD, Gaur S, Tsolia M, Scudder R, Howell R, Kesarwala H. Cytomegalovirus infection in children with aids. Rev Infect Dis. 1990;12:S820–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources