

Serological investigation of pneumonia as it presents to the physician's office
- PMID: 22346468
- PMCID: PMC3250773
- DOI: 10.1155/1993/435350
Serological investigation of pneumonia as it presents to the physician's office
Abstract
Purpose: To define the etiology of pneumonia, using a battery of serological tests, among patients presenting to physicians' offices in Cumberland County, Nova Scotia from July 2, 1989 to July 1, 1990.
Methods: Patients presenting to their physician's office with symptoms suggestive of pneumonia were invited to participate in the study by completing a questionnaire, having a chest radiograph and providing acute and convalescent phase serum samples. These serum samples were tested for antibodies to Mycoplasma pneumoniae, Coxiella burnetii, Legionella pneumophila, adenovirus, and influenza viruses A and B. Some of the samples were tested for antibodies to Chlamydia pneumoniae.
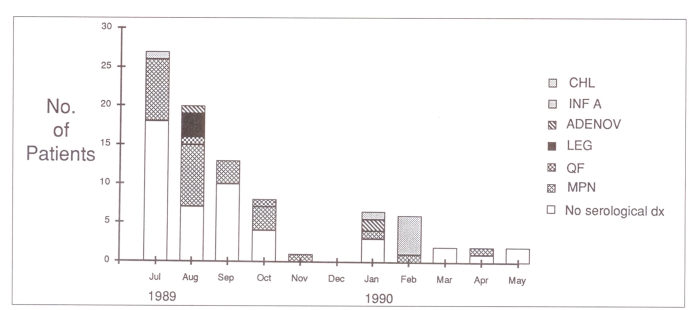
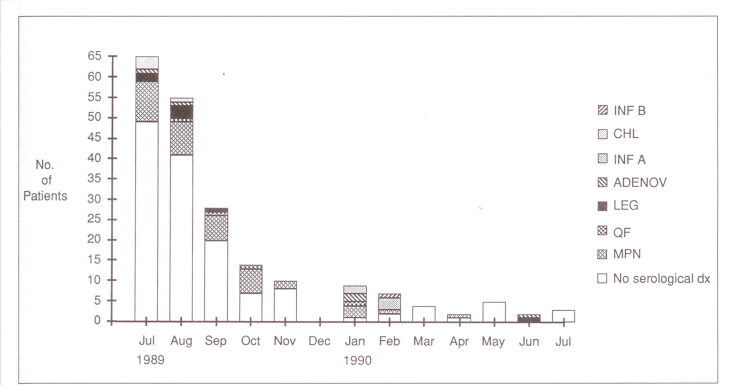
Results: Seventy-five of the inception cohort of 203 patients had a chest radiograph compatible with pneumonia, a completed questionnaire and acute and convalescent phase serum samples. There were 39 females and 36 males with a mean age of 41.7 years. Twenty-six (35%) were admitted to hospital. The mortality rate was 3%. Forty-five per cent had a diagnosis made by serology: M pneumoniae, 22 (29%); influenza A virus, five (7%); C burnetii, L pneumophila, adenovirus, two (3%) each.
Conclusions: While it is not possible to generalize about these findings because of ascertainment bias, the data suggest that M pneumoniae is a common cause of pneumonia presenting to a physician's office and that mortality is low in this group of patients.
Objectif:: Définir l’étiologie de la pneumonie à l’aide d’une batterie de tests sérologiques chez les patients qui se présentèrent dans les cabinets médicaux du comté de Cumberland (Nouvelle-Écosse) entre juillet 1989 et le 1er juillet 1990.
Méthodes:: Des patients se présentant au cabinet de leur médecin avec des symptômes évocateurs de pneumonie ont été invités à participer à l’étude en remplissant un questionnaire, en subissant une radiographie pulmonaire et en fournissant des spécimens sériques durant la phase aiguë et la convalescence. Ces échantillons de sérum ont été analysés à l’égard des anticorps dirigés contre Mycoplasma pneumoniae, Coxiella burnettii, Legionella pneumophila, l’adénovirus et les virus de l’influenza A et B. Certains échantillons ont été analysés à l’égard des anticorps anti-Chlamydia pneumoniae.
Résultats:: Soixante-quinze pour cent de la cohorte d’inception de 203 patients qui présentaient des signes radiologiques de pneumonie ont rempli le questionnaire et soumis des échantillons de sérum durant la phase aiguë et la convalescence. Il y avait 39 femmes et 36 hommes, dont la moyenne d’âge était de 41,7 ans. Vingt-six (35 %) ont été admis à l’hôpital. Le taux de mortalité a été de 3 %. Quarante-cinq pour cent ont vu leur diagnostic confirmé par des analyses sérologiques: M pneumoniae, 22 (29 %); virus de l’influenza 5 (7 %); C burnetii, L pneumophila, adénovirus, 2 (3 %) chacun.
Conclusions:: Bien que l’on ne puisse généraliser, nos données suggèrent que M pneumoniae est une cause fréquente de pneumonie parmi les patients qui se présentent chez leur médecin et le taux de mortalité est faible dans ce groupe de patients.
Keywords: Coxiella burnetii; Epidemiology; Legionella; Mycoplasma; Pneumonia.
Figures
References
-
- Bath JCJL, Boissard GPB, Calder MA, Moffat MAJ. Pneumonia in hospital practice in Edinburgh 1960–1962. Br J Dis Chest. 1964;58:1–16. - PubMed
-
- Mufson MA, Chang V, Gill V, Wood SC, Romansky MJ, Chanock RM. The role of viruses, mycoplasmas and bacteria in acute pneumonia in civilian adults. Am J Epidemiol. 1967;86:526–44. - PubMed
-
- Fekety FR, Jr, Caldwell J, Gump D, et al. Bacteria, viruses and mycoplasmas in acute pneumonia in adults. Am Rev Respir Dis. 1971;104:499–507. - PubMed
-
- Sullivan RJ, Jr, Dowdle WR, Marine WM, Hierholzer JD. Adult pneumonia in a general hospital: Etiology and host risk factors. Arch Intern Med. 1972;129:935–42. - PubMed
-
- Dorff GJ, Rytel MW, Farmer SG, Scanlon G. Etiologies and characteristic features of pneumonia in a municipal hospital. Am J Med Sci. 1973;266:349–58. - PubMed
LinkOut - more resources
Full Text Sources