

Characterisation of Clostridium difficile hospital ward-based transmission using extensive epidemiological data and molecular typing
- PMID: 22346738
- PMCID: PMC3274560
- DOI: 10.1371/journal.pmed.1001172
Characterisation of Clostridium difficile hospital ward-based transmission using extensive epidemiological data and molecular typing
Abstract
Background: Clostridium difficile infection (CDI) is a leading cause of antibiotic-associated diarrhoea and is endemic in hospitals, hindering the identification of sources and routes of transmission based on shared time and space alone. This may compromise rational control despite costly prevention strategies. This study aimed to investigate ward-based transmission of C. difficile, by subdividing outbreaks into distinct lineages defined by multi-locus sequence typing (MLST).
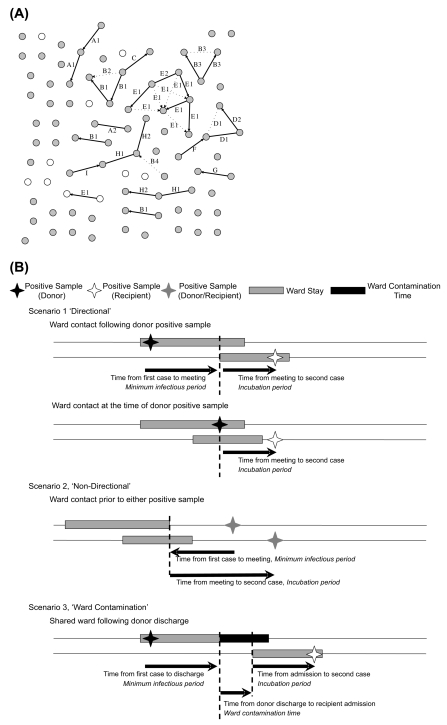
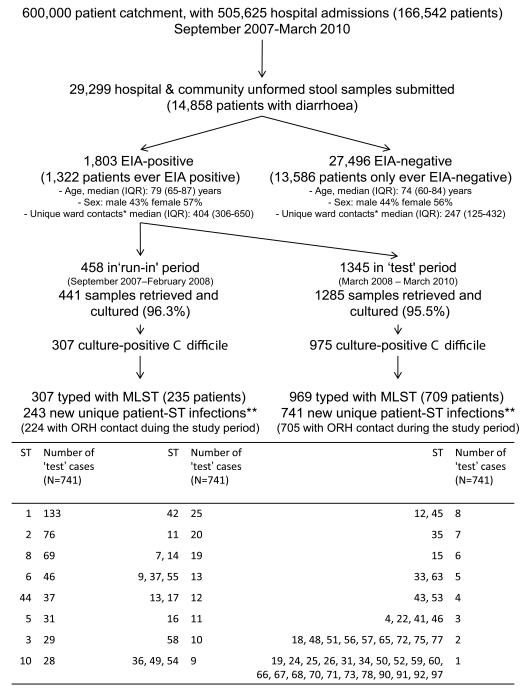
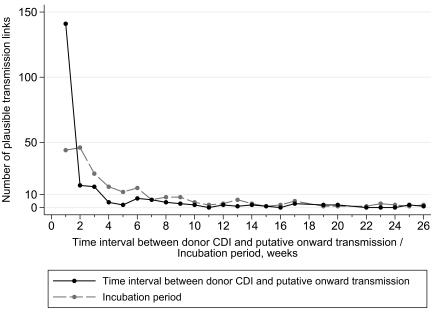
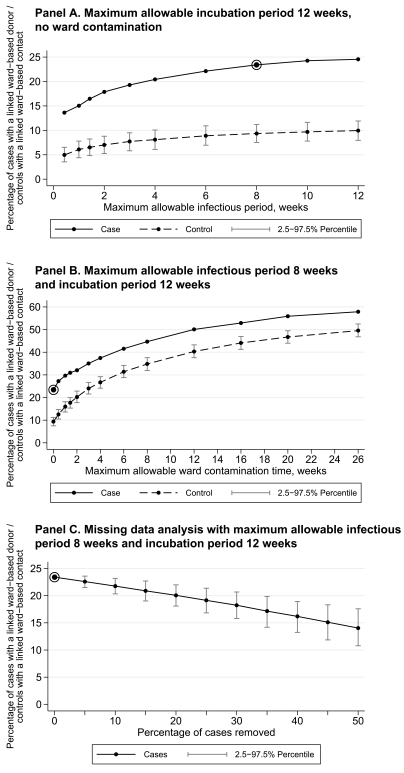
Methods and findings: All C. difficile toxin enzyme-immunoassay-positive and culture-positive samples over 2.5 y from a geographically defined population of ~600,000 persons underwent MLST. Sequence types (STs) were combined with admission and ward movement data from an integrated comprehensive healthcare system incorporating three hospitals (1,700 beds) providing all acute care for the defined geographical population. Networks of cases and potential transmission events were constructed for each ST. Potential infection sources for each case and transmission timescales were defined by prior ward-based contact with other cases sharing the same ST. From 1 September 2007 to 31 March 2010, there were means of 102 tests and 9.4 CDIs per 10,000 overnight stays in inpatients, and 238 tests and 15.7 CDIs per month in outpatients/primary care. In total, 1,276 C. difficile isolates of 69 STs were studied. From MLST, no more than 25% of cases could be linked to a potential ward-based inpatient source, ranging from 37% in renal/transplant, 29% in haematology/oncology, and 28% in acute/elderly medicine to 6% in specialist surgery. Most of the putative transmissions identified occurred shortly (≤ 1 wk) after the onset of symptoms (141/218, 65%), with few >8 wk (21/218, 10%). Most incubation periods were ≤ 4 wk (132/218, 61%), with few >12 wk (28/218, 13%). Allowing for persistent ward contamination following ward discharge of a CDI case did not increase the proportion of linked cases after allowing for random meeting of matched controls.
Conclusions: In an endemic setting with well-implemented infection control measures, ward-based contact with symptomatic enzyme-immunoassay-positive patients cannot account for most new CDI cases.
Conflict of interest statement
The institution of DWC and TEAP received per-case funding from Optimer Pharmaceuticals to support fidaxomicin trial patient expenses. DWC and TEAP also received honoraria from Optimer Pharmaceuticals for participation in additional meetings related to investigative planning for fidaxomicin. MHW has received honoraria for consultancy work, financial support to attend meetings and research funding from bioMerieux, Optimer, Novacta, Pfizer, Summit, The Medicines Company, and Viropharma. All other authors have declared that no competing interests exist.
Figures

Comment in
-
Clostridium: transmission difficile?PLoS Med. 2012 Feb;9(2):e1001171. doi: 10.1371/journal.pmed.1001171. Epub 2012 Feb 7. PLoS Med. 2012. PMID: 22346737 Free PMC article.
References
-
- Cohen SH, Gerding DN, Johnson S, Kelly CP, Loo VG, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the society for healthcare epidemiology of America (SHEA) and the infectious diseases society of America (IDSA). Infect Control Hosp Epidemiol. 2010;31:431–455. - PubMed
-
- Loo VG, Poirier L, Miller MA, Oughton M, Libman MD, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality. N Engl J Med. 2005;353:2442–2449. - PubMed
-
- McDonald LC, Killgore GE, Thompson A, Owens RC, Jr, Kazakova SV, et al. An epidemic, toxin gene-variant strain of Clostridium difficile. N Engl J Med. 2005;353:2433–2441. - PubMed
-
- Vonberg RP, Kuijper EJ, Wilcox MH, Barbut F, Tull P, et al. Infection control measures to limit the spread of Clostridium difficile. Clin Microbiol Infect. 2008;14(Suppl 5):2–20. - PubMed
-
- Muto CA, Blank MK, Marsh JW, Vergis EN, O'Leary MM, et al. Control of an outbreak of infection with the hypervirulent Clostridium difficile BI strain in a university hospital using a comprehensive “bundle” approach. Clin Infect Dis. 2007;45:1266–1273. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
