

Non-invasive detection of pulmonary pathogens in ventilator-circuit filters by PCR
- PMID: 22347523
- PMCID: PMC3276378
Non-invasive detection of pulmonary pathogens in ventilator-circuit filters by PCR
Abstract
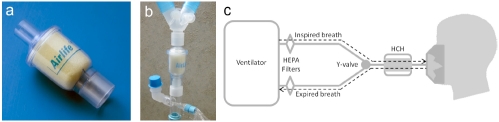
Ventilator associated pneumonia is a common and costly complication in critically ill and injured surgical patients. The diagnosis of pneumonia remains problematic and non-specific. Using clinical criteria, a diagnosis of pneumonia is typically not made until an infection is well established. Semi-quantitative cultures of endotracheal aspirate and broncho-alveolar lavage are employed to improve the accuracy of diagnosis but are invasive and require time for culture results to become available. We report data that show that an inexpensive, rapid and non-invasive alternative may exist. In particular we show that: 1). Bio-aerosols evolved in the breath of ventilated patients and captured in the hygroscopic condenser humidifier filter of the ventilator circuit contain pathogenic micro-organisms. 2). The number (CFU/ml) and identity (Genus, species) of the pathogens in the aerosol samples can rapidly and inexpensively be determined by PCR. 3). Data from a convenience sample of filters correlate with clinical findings from standard microbiological methods such as broncho-alveolar lavage. The evaluation of the bacterial load evolved in exhaled breath by PCR is amenable to repeated sampling. Since increasing bacterial burden is believed to correlate with the establishment of infection, the use of quantitative PCR may provide a method to rapidly, inexpensively, and effectively detect and diagnose the early onset of pneumonia and identify pathogens involved.
Keywords: BAL; HCH; HME; Pneumonia; VAP; infection.
Figures
References
-
- Richards MJ, Edwards JR, Culver DH, Gaynes R. Nosocomial infections in medical intensive care units in the united states. Critical Care Medicine. 1999;27:887–892. - PubMed
-
- American Thoracic Society, Guidelines for the management of adults with hospital-acquired, ventilator associated and healthcare associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416. - PubMed
-
- Iregui M, Ward S, Sherman G, Fraser VJ, Kollef MH. Clinical Importance of Delays in the Initiation of Appropriate Antibiotic Treatment for Ventilator-Associated Pneumonia. Chest. 2002;122:262–268. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources