Multivisceral resection for locally advanced rectal cancer: adequate length of distal resection margin
- PMID: 22347710
- PMCID: PMC3278640
- DOI: 10.4174/jkss.2012.82.2.87
Multivisceral resection for locally advanced rectal cancer: adequate length of distal resection margin
Abstract
Purpose: Locally advanced rectal cancer may require an intraoperative decision regarding curative multivisceral resection (MVR) of adjacent organs. In bulky tumor cases, ensuring sufficient distal resection margin (DRM) for achievement of oncologic safety is very difficult. This study is designed to evaluate the adequate length of DRM in multiviscerally resected rectal cancer.
Methods: A total of 324 patients who underwent curative low anterior resection for primary pT3-4 rectal cancer between 1995 and 2004 were identified from a prospectively collected colorectal database.
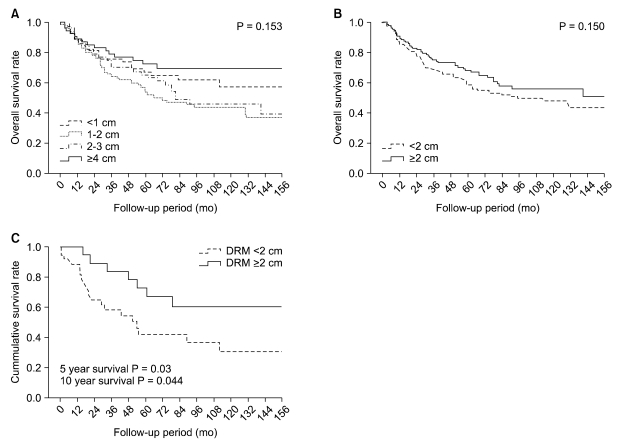
Results: Short lengths of DRM (≤1 cm) did not compromise essentially poor oncologic outcomes in locally advanced rectal cancer (P = 0.736). However, especially in rectal cancers invading adjacent organs, DRM of less than 2 cm showed poor survival outcome. In 5-year and 10-year survival analysis of MVR, a shorter DRM (<2 cm) showed 41.9% and 30.5%, although a longer DRM (≥2 cm) showed 72.4% and 60.2% (P = 0.03, 0.044). In multivariate analysis of MVR, poorly differentiated histology, ulceroinfiltrative growth of tumor, and short DRM (<2 cm) were significant factors for prediction of poor survival outcome, although short DRM was not significantly related to local and systemic recurrence.
Conclusion: In locally advanced rectal cancer of pT3-4, a short length of DRM (≤1 cm) did not compromise essentially poor oncologic outcome. In rectal cancers invading adjacent organs and requiring MVR, a shorter DRM (<2 cm) was found to be related to poor survival outcome.
Keywords: Distal resection margin; Locally advanced rectal cancer; Multivisceral resection.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures

Similar articles
-
Oncologic outcomes in rectal cancer patients with a ≤1-cm distal resection margin.Int J Colorectal Dis. 2017 Mar;32(3):325-332. doi: 10.1007/s00384-016-2708-1. Epub 2016 Nov 29. Int J Colorectal Dis. 2017. PMID: 27900522
-
Adequate length of the distal resection margin in rectal cancer: from the oncological point of view.J Gastrointest Surg. 2010 Aug;14(8):1331-7. doi: 10.1007/s11605-010-1165-3. Epub 2010 Feb 9. J Gastrointest Surg. 2010. PMID: 20143273 Review.
-
Oncologic outcomes in rectal cancer with close distal resection margins: a retrospective analysis.Ann Surg Treat Res. 2015 Jul;89(1):23-9. doi: 10.4174/astr.2015.89.1.23. Epub 2015 Jun 11. Ann Surg Treat Res. 2015. PMID: 26131441 Free PMC article.
-
Multivisceral resection of advanced colon and rectal cancer: a prospective multicenter observational study with propensity score analysis of the morbidity, mortality, and survival.Innov Surg Sci. 2023 Nov 27;8(2):61-72. doi: 10.1515/iss-2023-0027. eCollection 2023 Jun. Innov Surg Sci. 2023. PMID: 38058778 Free PMC article.
-
Laparoscopic and robotic multivisceral resection in colorectal cancer: A case series and systematic review.Asian J Endosc Surg. 2023 Jul;16(3):343-353. doi: 10.1111/ases.13162. Epub 2023 Jan 4. Asian J Endosc Surg. 2023. PMID: 36599163
Cited by
-
Outcomes of pelvic exenteration for recurrent or primary locally advanced colorectal cancer.Ann Surg Treat Res. 2015 Sep;89(3):131-7. doi: 10.4174/astr.2015.89.3.131. Epub 2015 Aug 24. Ann Surg Treat Res. 2015. PMID: 26366382 Free PMC article.
-
An anatomical study on intersphincteric space related to intersphincteric resection for ultra-low rectal cancer.Updates Surg. 2022 Apr;74(2):439-449. doi: 10.1007/s13304-022-01238-0. Epub 2022 Jan 19. Updates Surg. 2022. PMID: 35044586
References
-
- Lopez MJ. Multivisceral resections for colorectal cancer. J Surg Oncol. 2001;76:1–5. - PubMed
-
- National Comprehensive Cancer Network (NCCN) Colon cancer and rectal cancer guidelines, ver. 1. Washington: National Comprehensive Cancer Network (NCCN); 2007. - PubMed
-
- Moore HG, Riedel E, Minsky BD, Saltz L, Paty P, Wong D, et al. Adequacy of 1-cm distal margin after restorative rectal cancer resection with sharp mesorectal excision and preoperative combined-modality therapy. Ann Surg Oncol. 2003;10:80–85. - PubMed
-
- Kwok SP, Lau WY, Leung KL, Liew CT, Li AK. Prospective analysis of the distal margin of clearance in anterior resection for rectal carcinoma. Br J Surg. 1996;83:969–972. - PubMed
LinkOut - more resources
Full Text Sources