

Computed tomography of complicated Meckel's diverticulum in adults: a pictorial review
- PMID: 22347905
- PMCID: PMC3259399
- DOI: 10.1007/s13244-010-0017-8
Computed tomography of complicated Meckel's diverticulum in adults: a pictorial review
Abstract
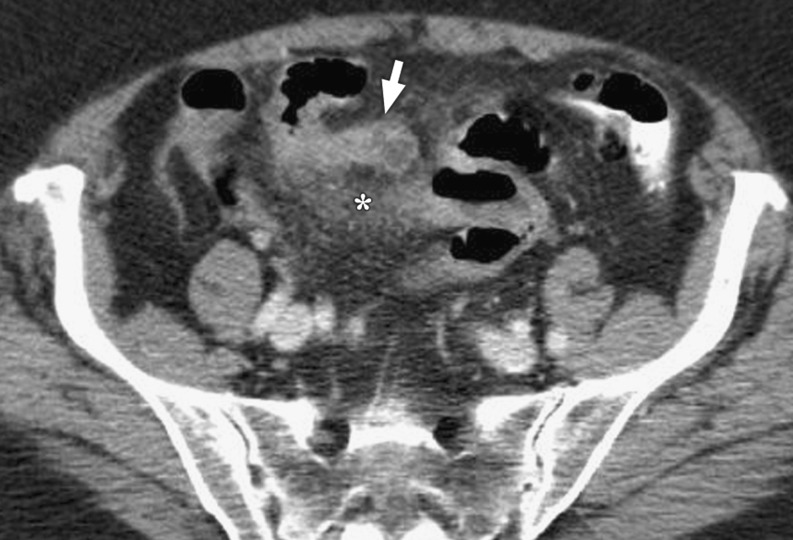
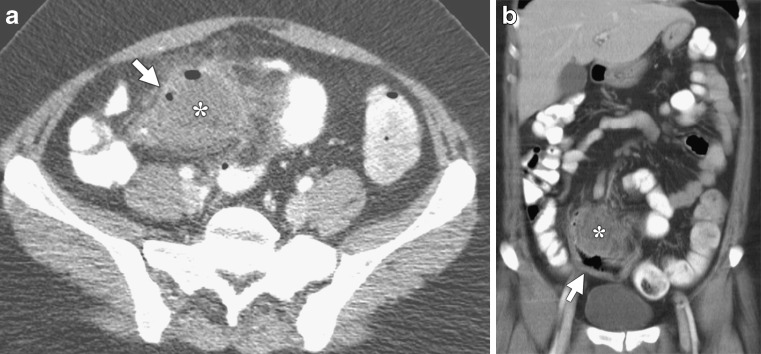
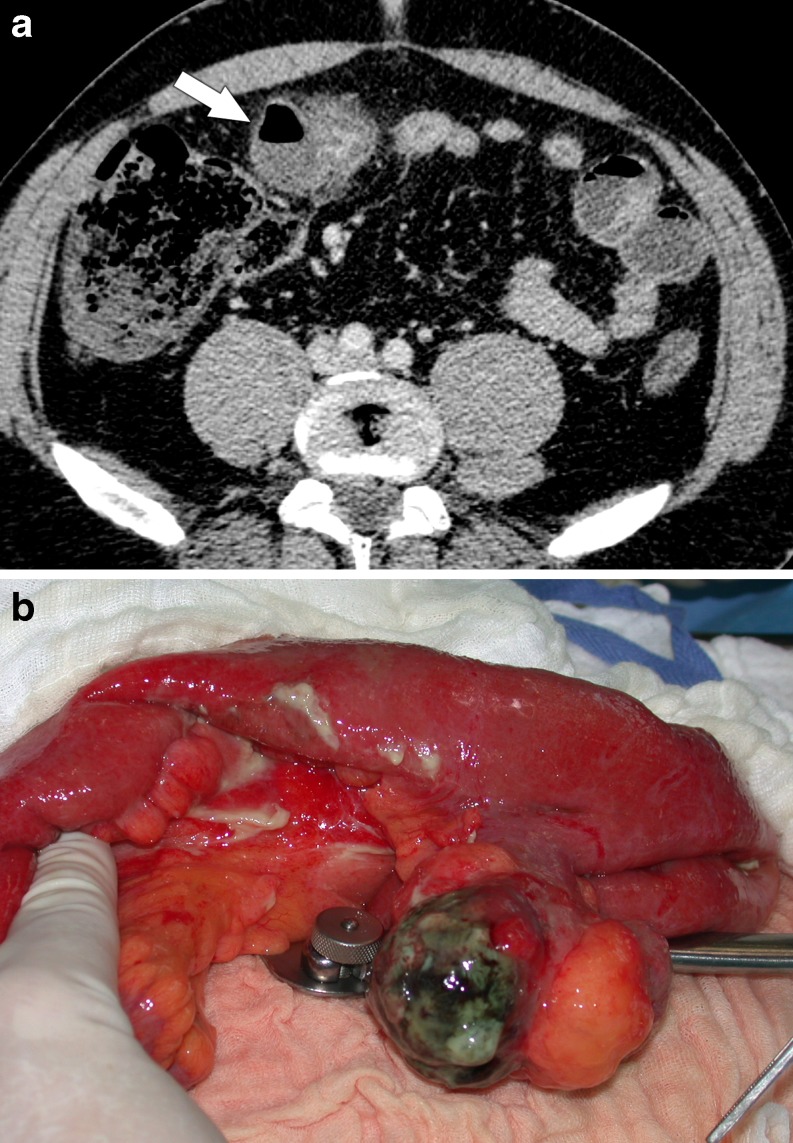
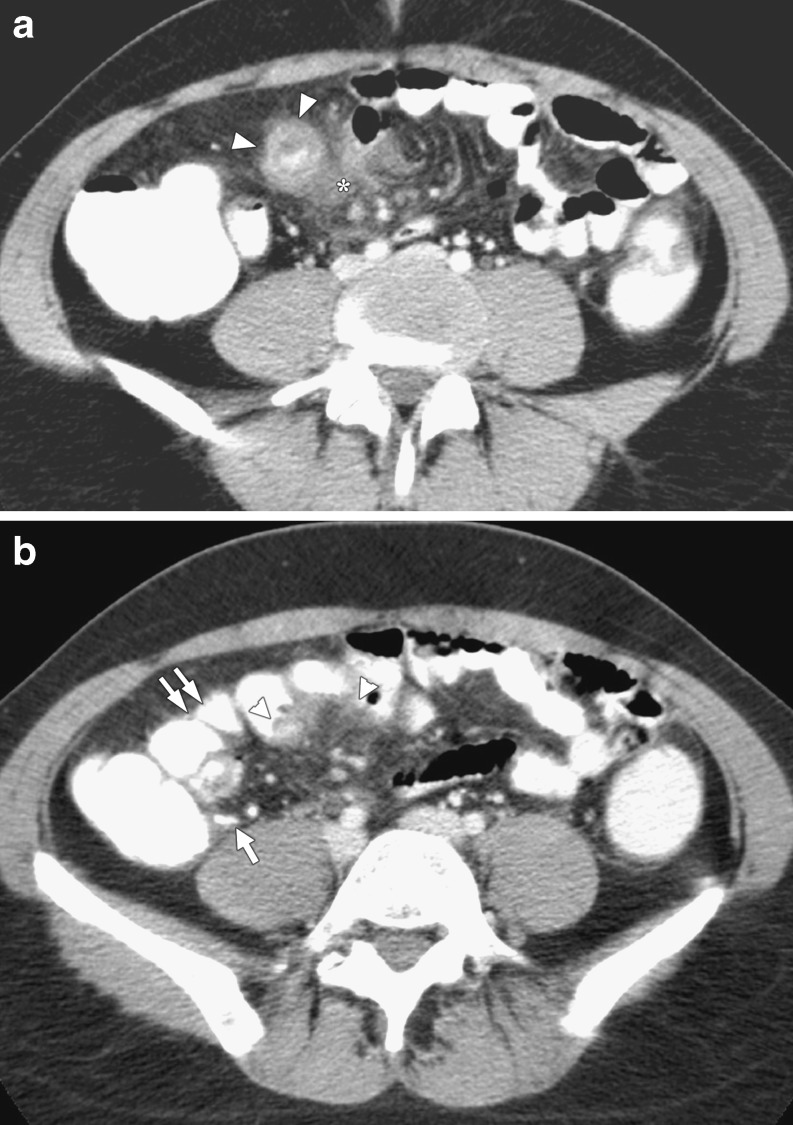
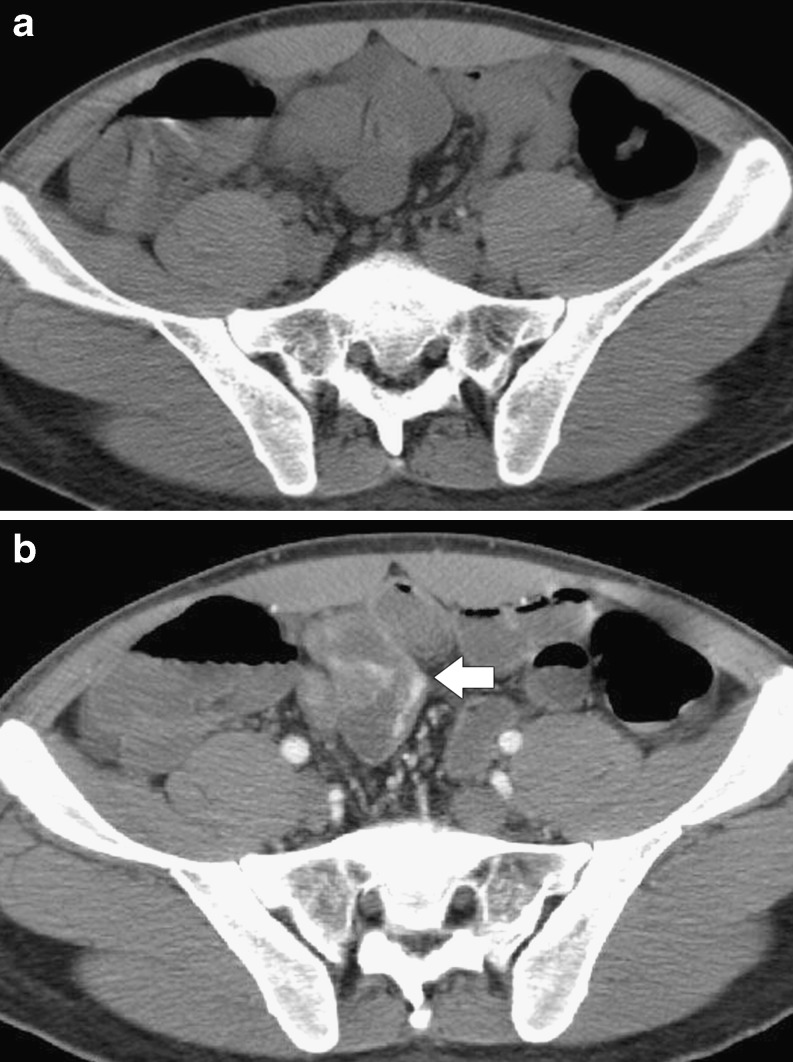
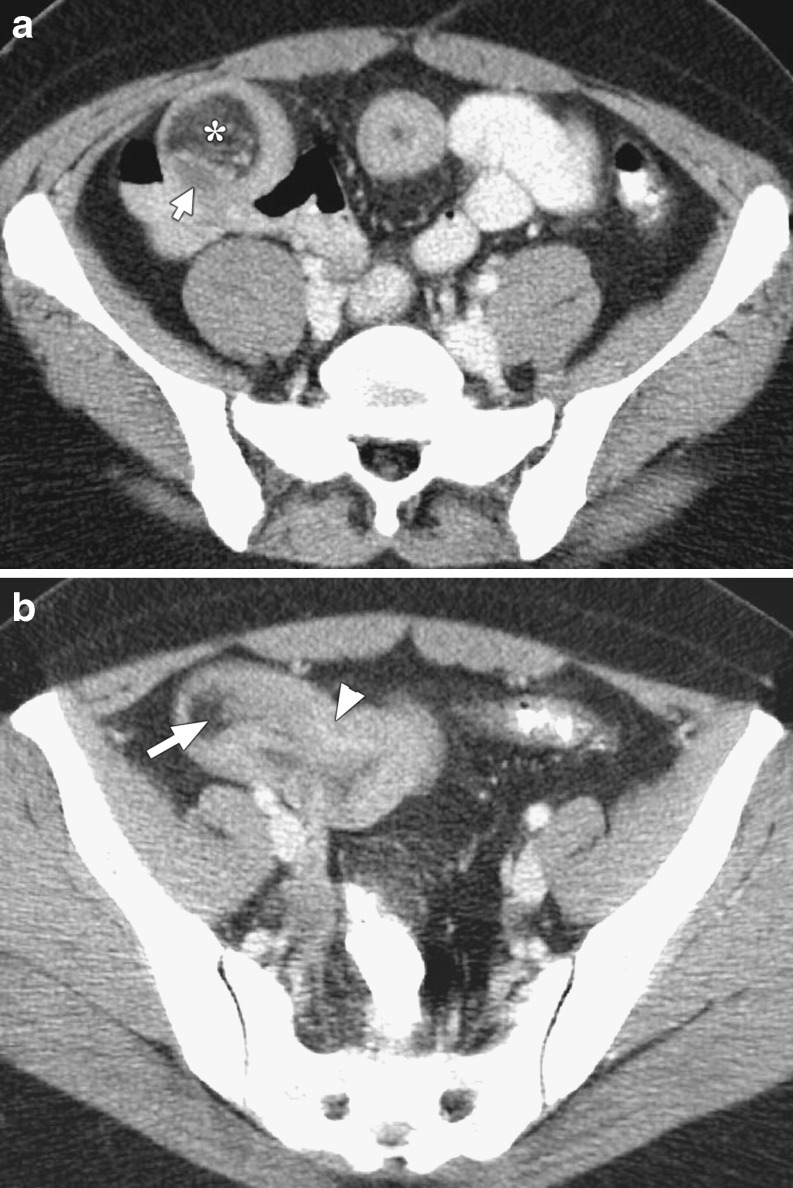
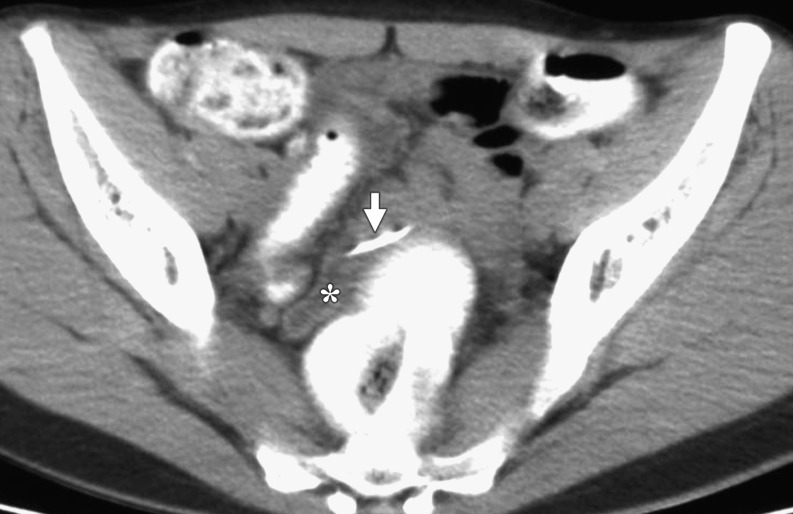
OBJECTIVE: To show various CT aspects of complicated Meckel's diverticulum in adult patients to facilitate the preoperative diagnosis of this rare pathology in emergency settings. METHODS: A computer search of medical records over a 15 year period identified 23 adult patients who underwent surgery for acute abdomen generated by a complicated Meckel's diverticulum. CT images available for review were analyzed, and some specific patterns leading to the diagnosis of complicated Meckel's diverticulum are presented in this review. RESULTS: Complications were related to inflammation (14 patients), bleeding (5 patients), intestinal obstruction (3 patients), and penetrating foreign body (1 patient). The presence of a Meckel's diverticulum was usually suggested at CT scan by an abnormal outpouching, blind-ending digestive structure connected to the terminal ileum by a neck of variable caliber. Depending on the type of complications, the diverticulum was surrounded by mesenteric inflammatory changes, or presented as a localized fluid or air-fluid collection contiguous with the terminal ileum. The diverticulum was also the source of active bleeding or acted as the lead point to intestinal obstruction or intussusception. CONCLUSION: CT findings of complicated Meckel's diverticulum are polymorphic and should be considered in the evaluation of adult patients with acute abdomen.
Figures




References
-
- Rossi P, Gourtsoyiannis N, Bezzi M, Raptopoulos V, Massa R, Capanna G, Pedicini V, Coe M. Meckel's diverticulum: imaging diagnosis. AJR Am J Roentgenol. 1996;166:567–573. - PubMed
LinkOut - more resources
Full Text Sources