

Flying through congested airspaces: imaging of chronic rhinosinusitis
- PMID: 22347913
- PMCID: PMC3259331
- DOI: 10.1007/s13244-010-0030-y
Flying through congested airspaces: imaging of chronic rhinosinusitis
Abstract
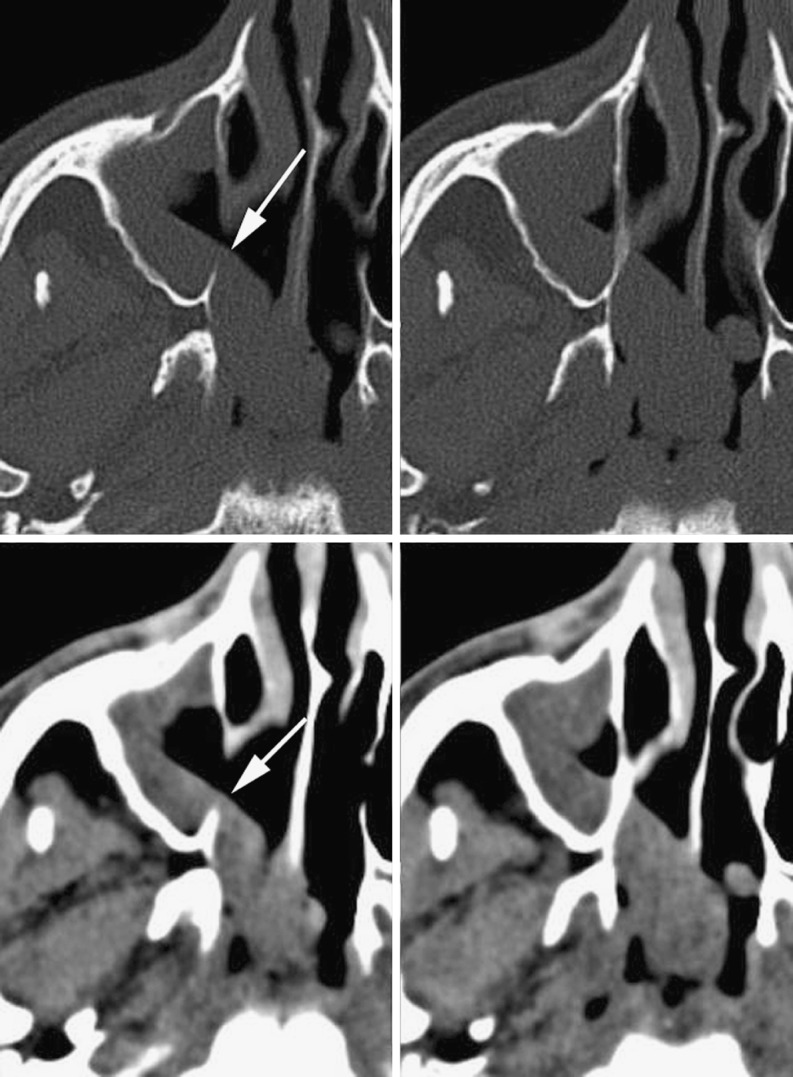
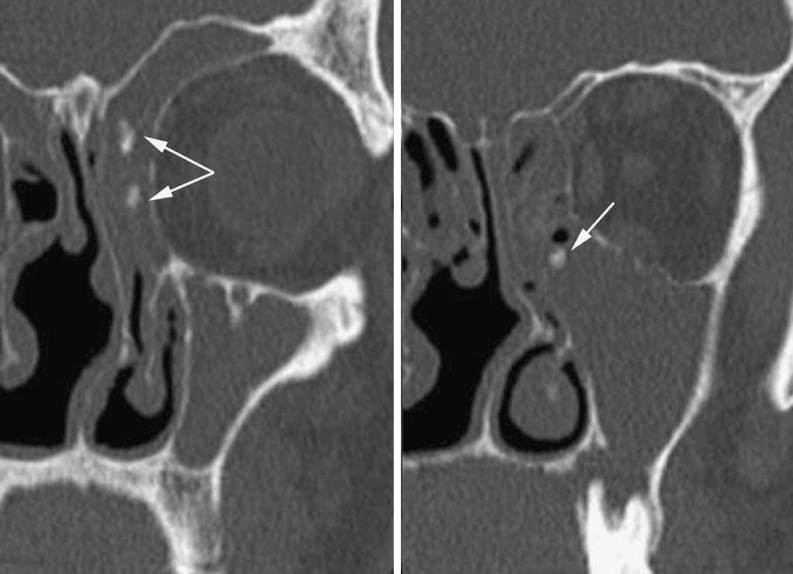
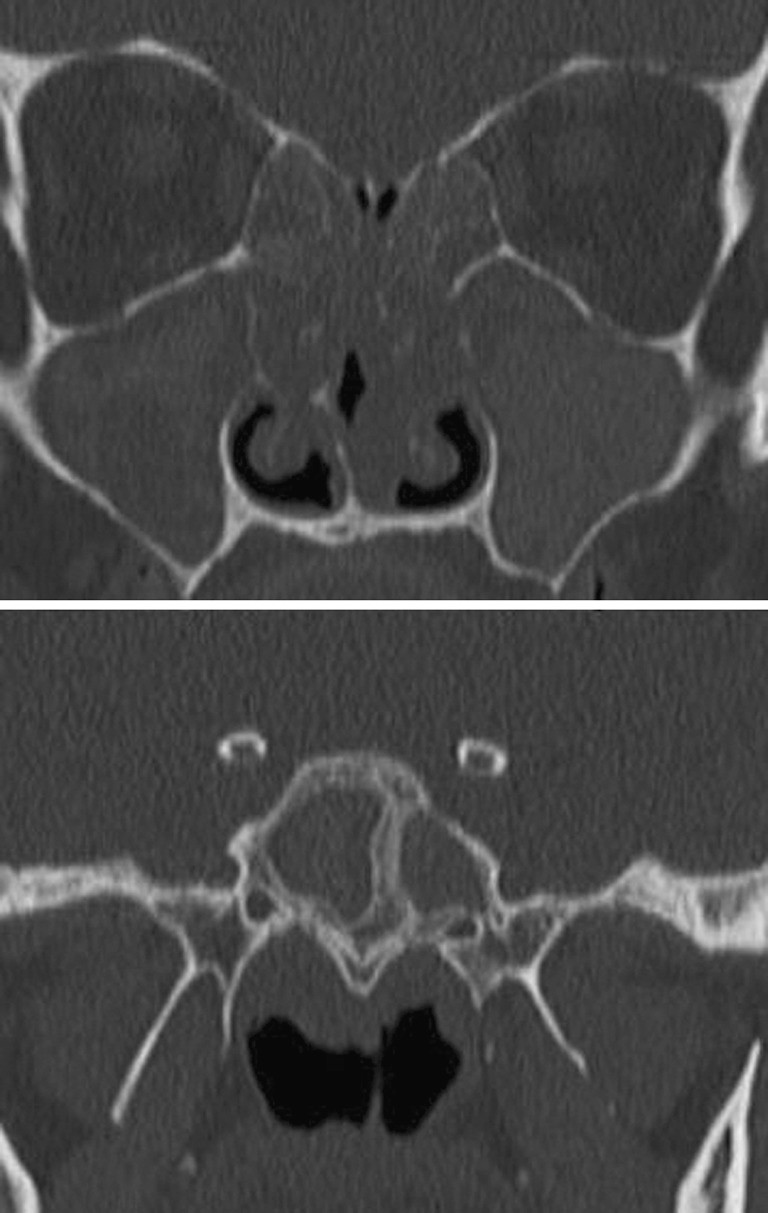
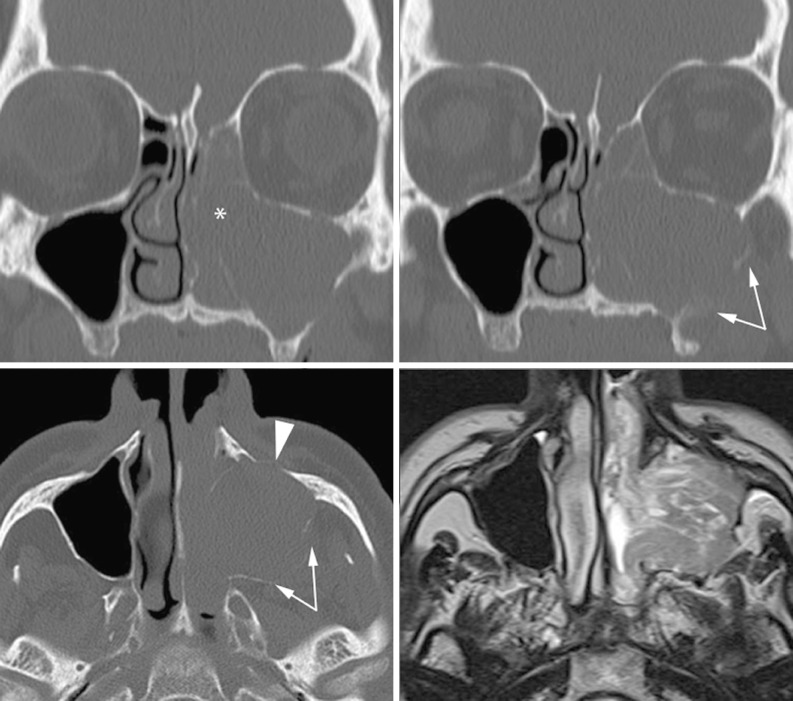
The complex regional anatomy of the nose and paranasal sinuses makes the interpretation of imaging studies of these structures intimidating to many radiologists. This paper aims to provide a key to interpretation by presenting a simplified approach to the functional anatomy of the paranasal sinuses and their most common (and most relevant) variants. This knowledge is basic for the full understanding of chronic rhinosinusitis and its computed tomography (CT) patterns. As fungal infections may be observed in the setting of chronic rhinosinusitis, these are also discussed. Chronic sinus inflammation produces bone changes, clearly depicted on CT images. Finally, clues to suspecting neoplastic lesions underlying inflammatory sinus conditions are provided.
Figures








References
LinkOut - more resources
Full Text Sources
Research Materials