

Kawasaki disease: a review with emphasis on cardiovascular complications
- PMID: 22347918
- PMCID: PMC3259313
- DOI: 10.1007/s13244-010-0035-6
Kawasaki disease: a review with emphasis on cardiovascular complications
Abstract
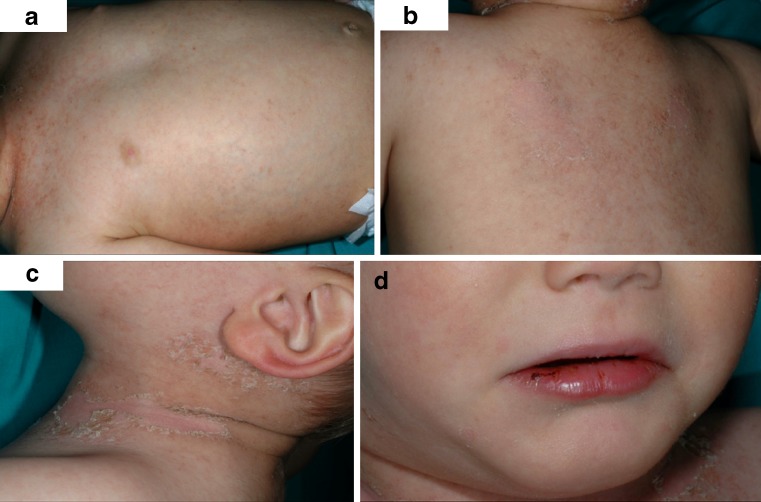
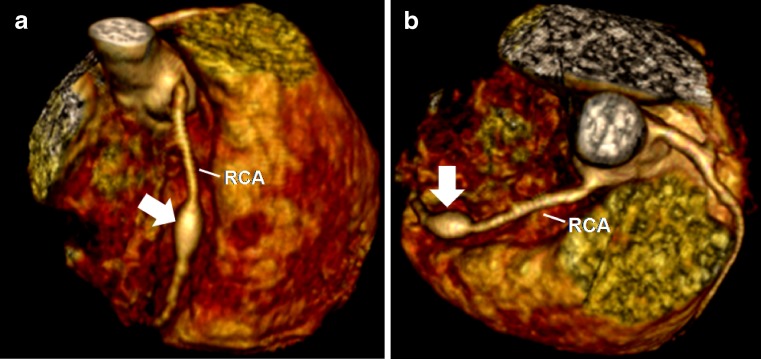
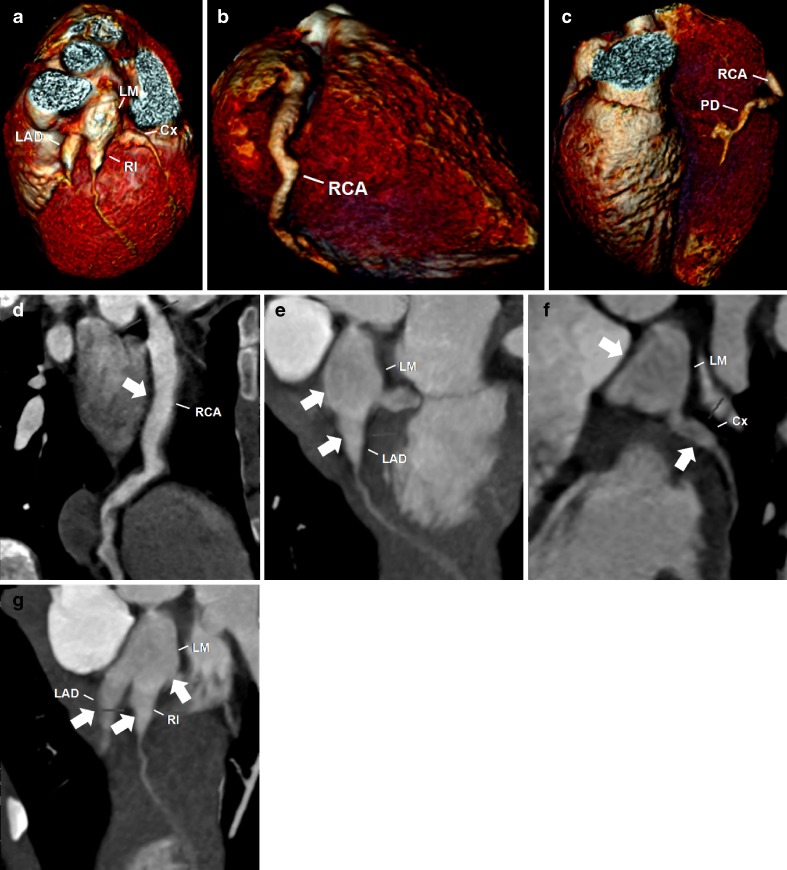
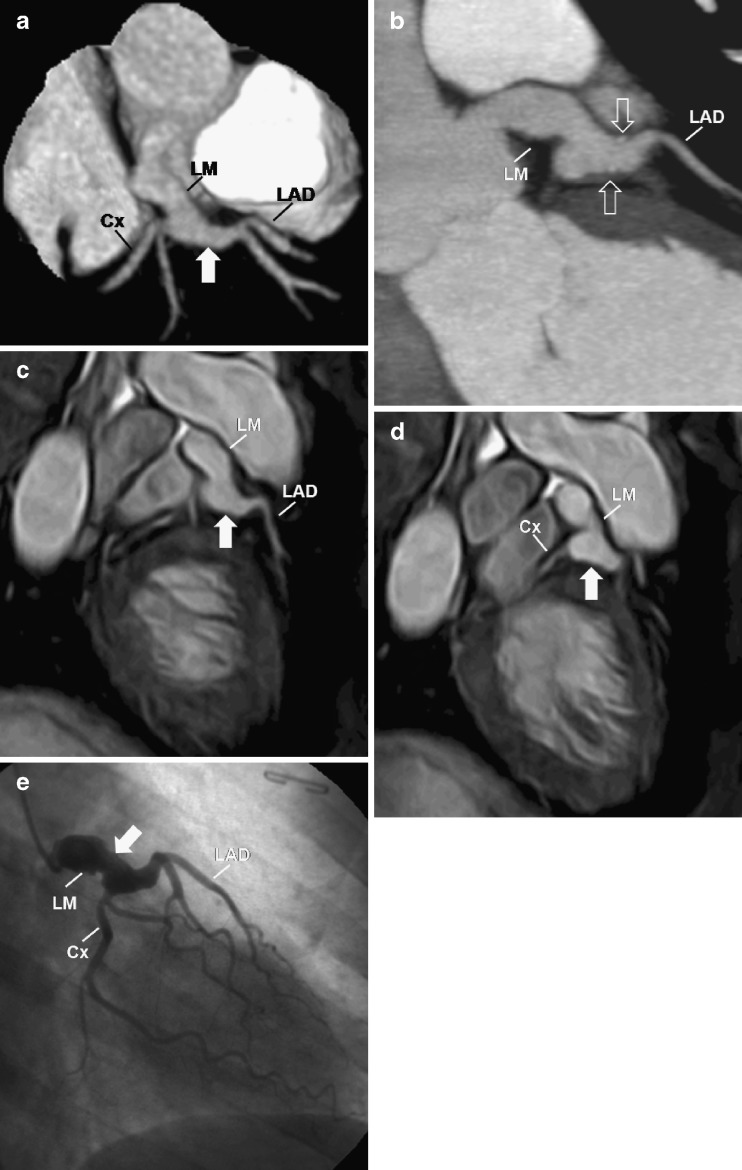
Kawasaki disease (KD) is an acute systemic vasculitis that is currently the leading cause of acquired heart disease in childhood in the United States. Cardiovascular complications are the major cause of morbidity, are responsible for virtually all deaths from KD and should be evaluated as soon as possible after the acute phase to establish the baseline status, in order to predict disease progression and determine adequate treatment. In selected patients, electrocardiography (ECG)-gated cardiac computed tomography (CT) and magnetic resonance (MR) imaging are valuable non-invasive techniques that can be used to help diagnose the cardiovascular complications associated with KD. In this article, we review the epidemiology, aetiology and pathogenesis, histopathology, clinical features, cardiovascular complications and imaging, focusing on the role of cardiac CT and MR on the initial assessment and follow-up of the cardiovascular complications of KD.
Figures
References
-
- Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Circulation. 2004;110:2747–2771. doi: 10.1161/01.CIR.0000145143.19711.78. - DOI - PubMed
-
- Chung C, Stein L. Kawasaki disease: a review. Radiology. 1998;208:25–33. - PubMed
LinkOut - more resources
Full Text Sources