

Technical aspects of CT imaging of the spine
- PMID: 22347928
- PMCID: PMC3259341
- DOI: 10.1007/s13244-010-0047-2
Technical aspects of CT imaging of the spine
Abstract
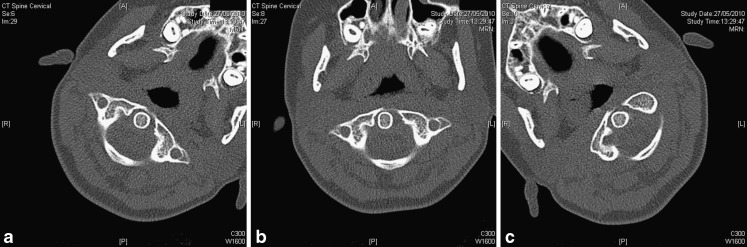
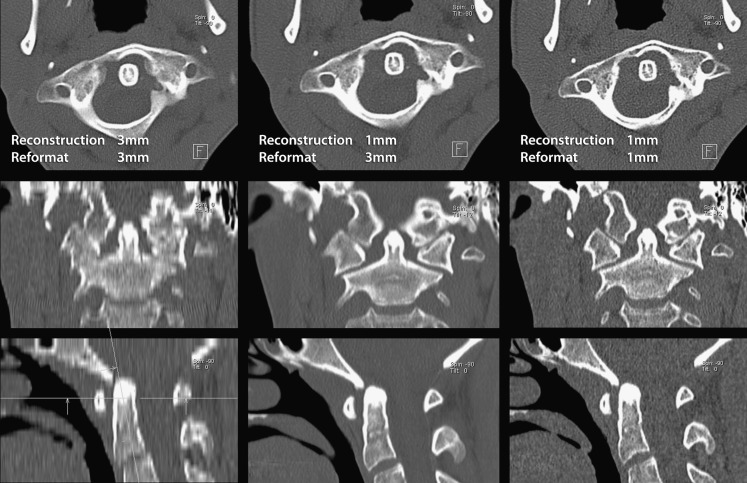
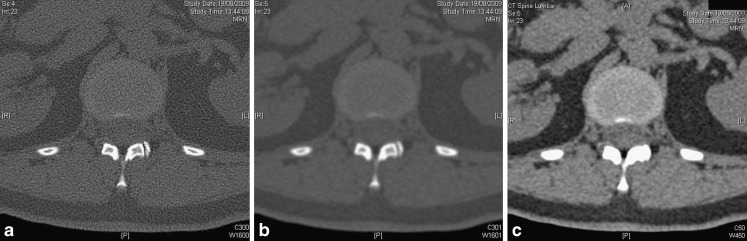
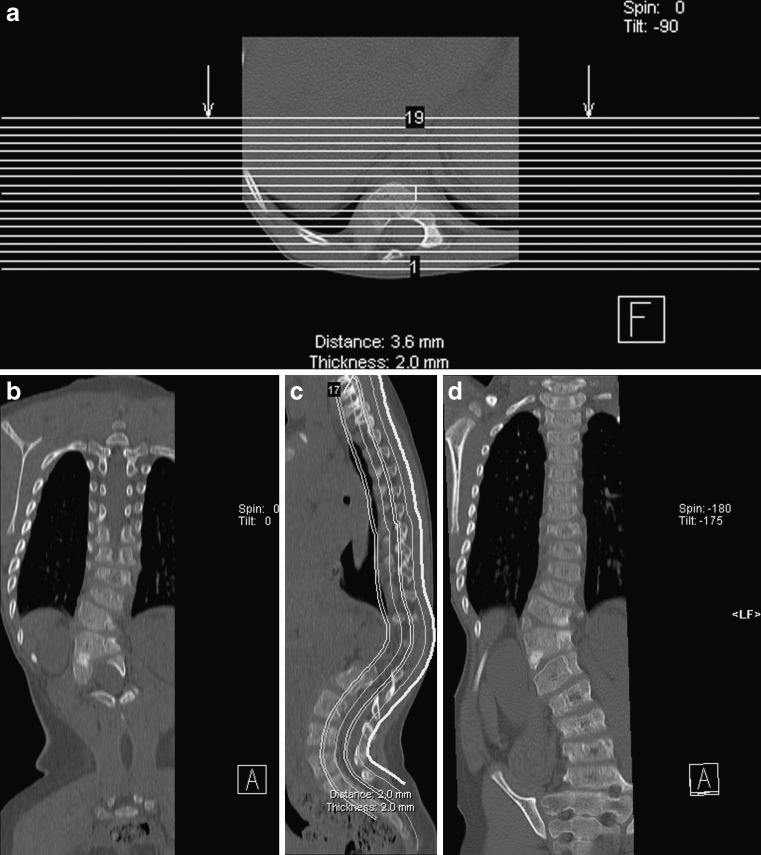
This review article discusses technical aspects of computed tomography (CT) imaging of the spine. Patient positioning, and its influence on image quality and movement artefact, is discussed. Particular emphasis is placed on the choice of scan parameters and their relation to image quality and radiation burden to the patient. Strategies to reduce radiation burden and artefact from metal implants are outlined. Data acquisition, processing, image display and steps to reduce artefact are reviewed. CT imaging of the spine is put into context with other imaging modalities for specific clinical indications or problems. This review aims to review underlying principles for image acquisition and to provide a rough guide for clinical problems without being prescriptive. Individual practice will always vary and reflect differences in local experience, technical provisions and clinical requirements.
Figures



References
-
- Richards PJ, George J, Metelko M, et al. Spine computed tomography doses and cancer induction. Spine (Phila Pa 1976) 2010;35(4):430–433. - PubMed
LIST 1: websites with CT imaging protocols (alphabetical order)
LinkOut - more resources
Full Text Sources