

CT findings of misleading features of colonic diverticulitis
- PMID: 22347935
- PMCID: PMC3259374
- DOI: 10.1007/s13244-010-0051-6
CT findings of misleading features of colonic diverticulitis
Abstract
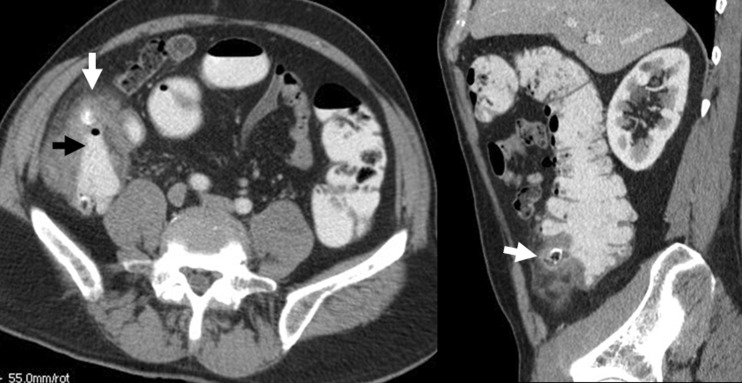
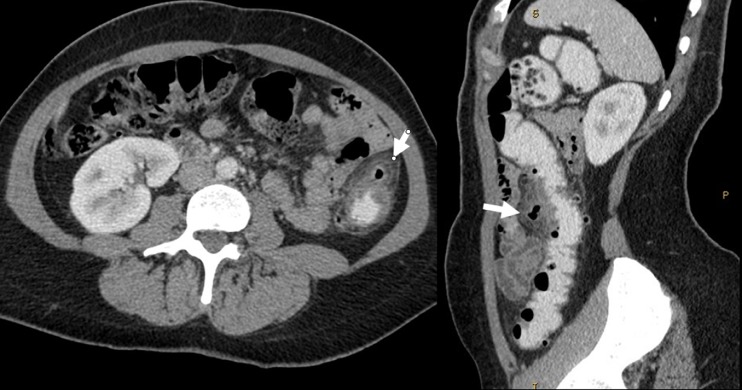
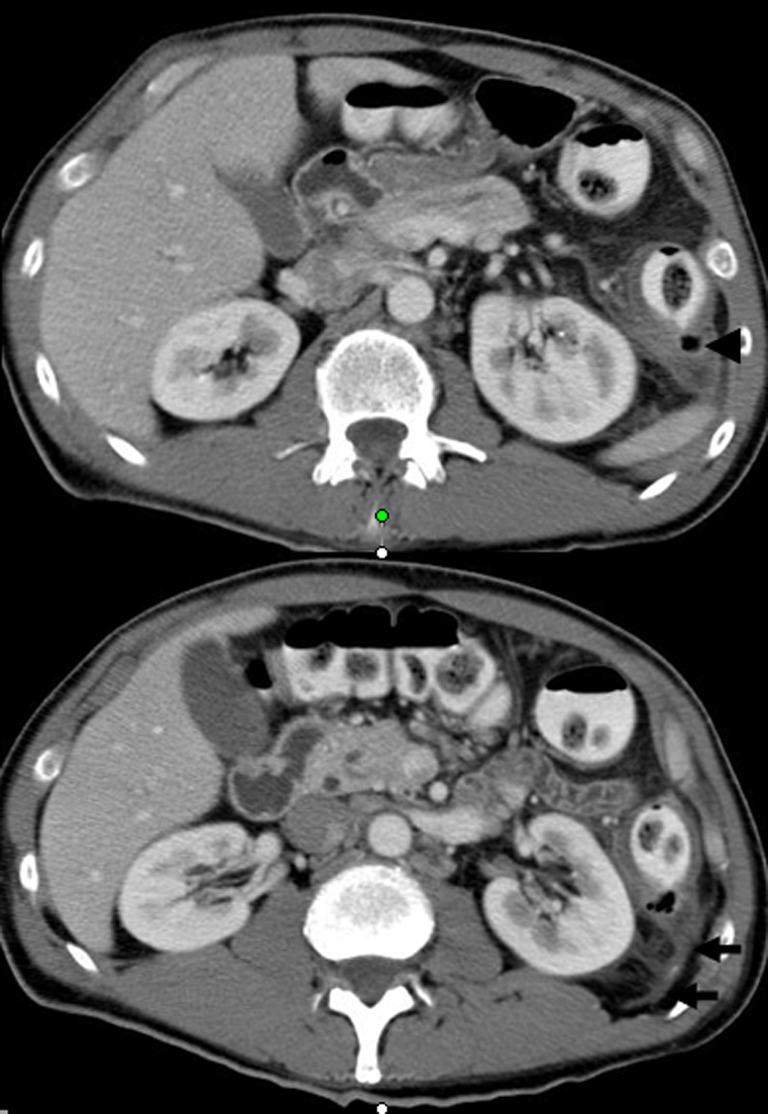
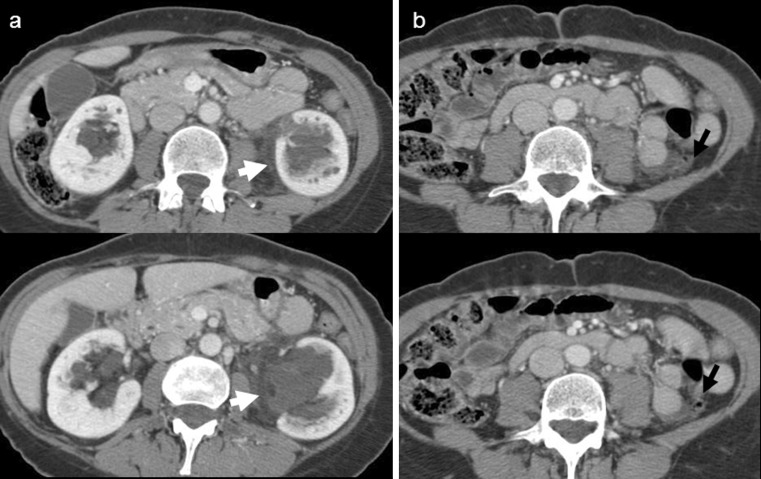
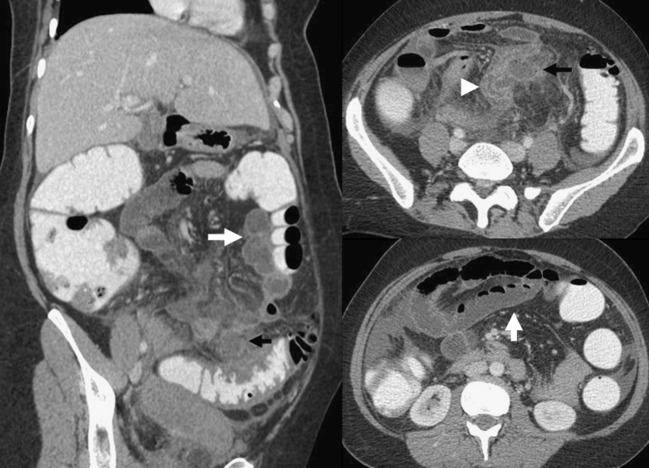
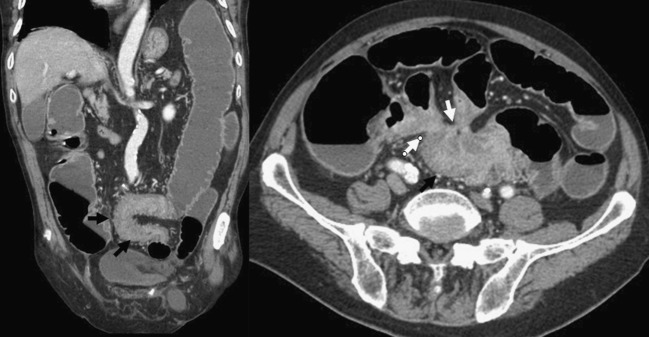
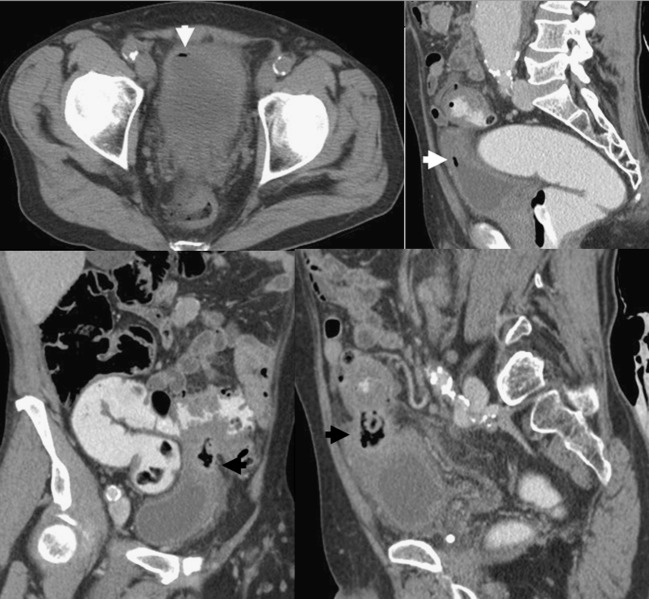
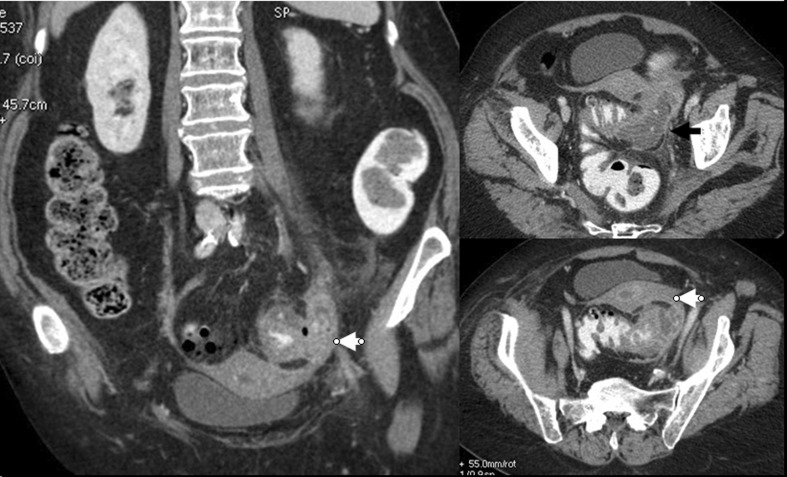
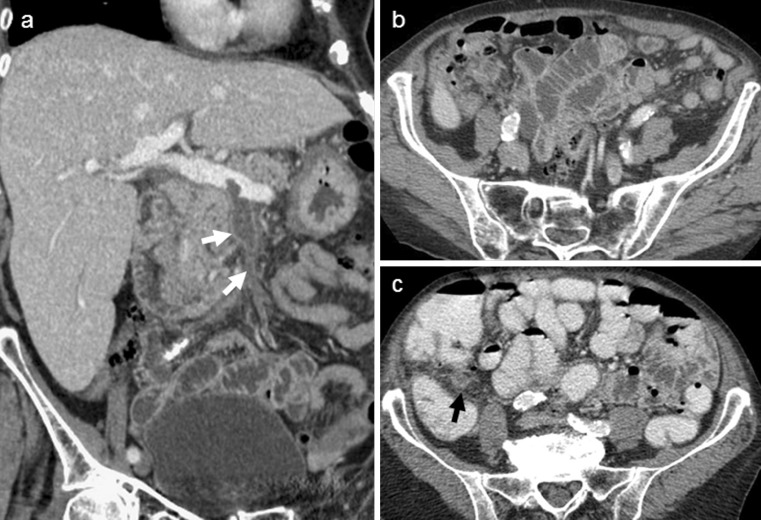
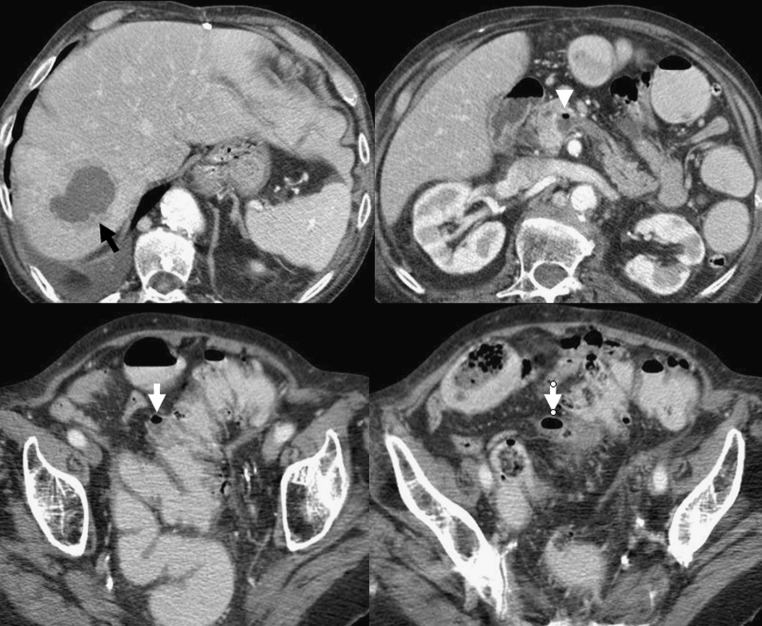
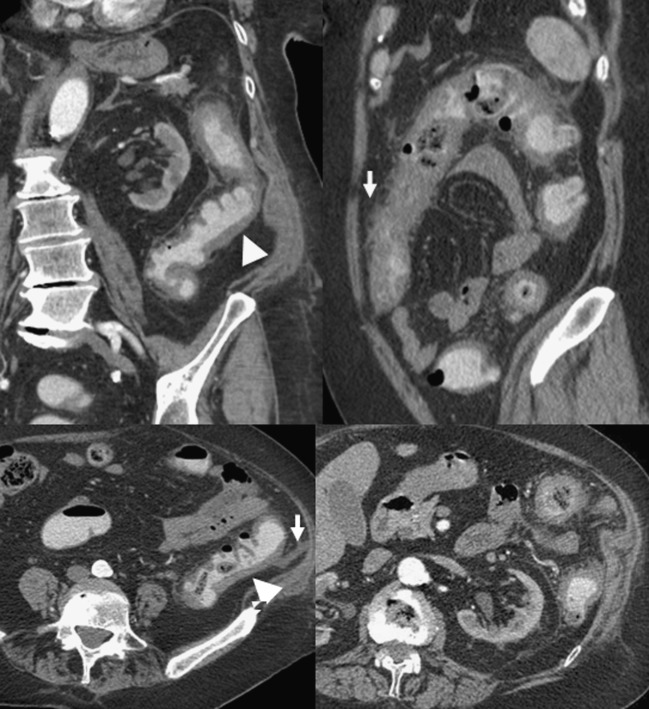
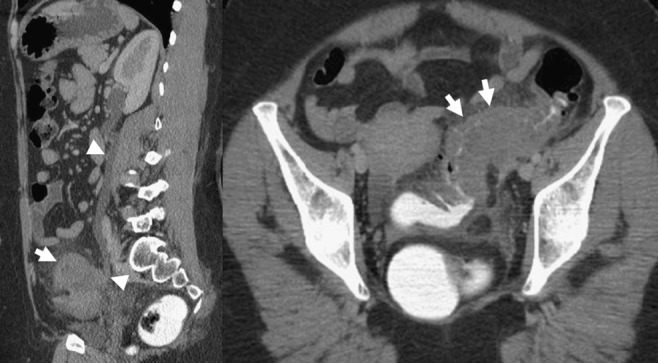
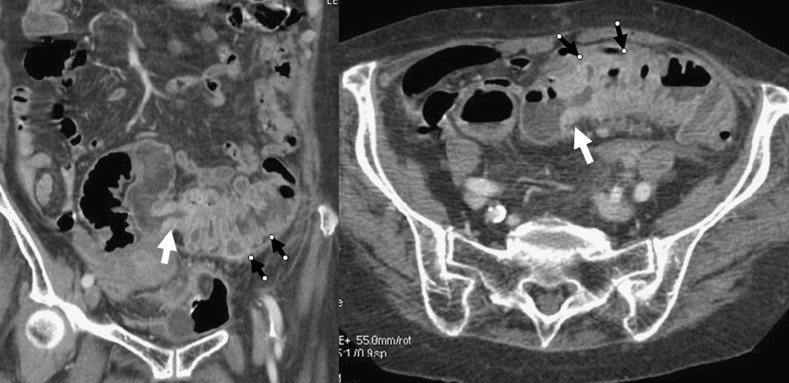
Colonic diverticulitis (CD) is a common entity whose diagnosis is particularly based on computed tomography (CT) examination, which is the imaging technique of choice. However, unusual CT findings of CD may lead to several difficulties and potential pitfalls: due to technical errors in the management of the CT examination, due to the anatomical situation of the diseased colon, in diagnosing unusual complications that may concern the gastrointestinal tract, intra- and retroperitoneal viscera or the abdominal wall, and in differentiating CD from other abdominal inflammatory and infectious conditions or colonic cancer. The aim of this work is to delineate the pitfalls of CT imaging and illustrate misleading CT features in patients with suspected CD.
Figures






References
-
- Zins M, Bruel JM, Pochet P, Regent D, Loiseau D. Question 1. What is the diagnostic value of the different tests for simple and complicated diverticulitis? What diagnostic strategy should be used? Gastroentérol Clin Biol. 2007;31:3S15–3S19. - PubMed
-
- Balthazar EJ, Megibow A, Schinella RA, Gordon R. Limitations in the CT diagnosis of acute diverticulitis: comparison of CT, contrast enema, and pathologic findings in 16 patients. AJR Am J Roentgenol. 1990;154:281–285. - PubMed
LinkOut - more resources
Full Text Sources