

doi: 10.1007/s13244-010-0060-5.
Epub 2011 Jan 9.
The crazy-paving pattern: a radiological-pathological correlation
- PMID: 22347941
- PMCID: PMC3259383
- DOI: 10.1007/s13244-010-0060-5
Item in Clipboard
The crazy-paving pattern: a radiological-pathological correlation
Insights Imaging.
2011 Apr.
Abstract
The crazy-paving pattern is a linear pattern superimposed on a background of ground-glass opacity, resembling irregularly shaped paving stones. The crazy-paving pattern is initially described as the pathognomonic sign of alveolar proteinosis. Nowadays this pattern is a common finding on high-resolution CT imaging, and can be seen in a number of acute and chronic diseases. The purpose of this paper is to illustrate different diseases that cause this crazy-paving pattern and to correlate the radiological findings from computed tomography with the histopathological findings.
Figures
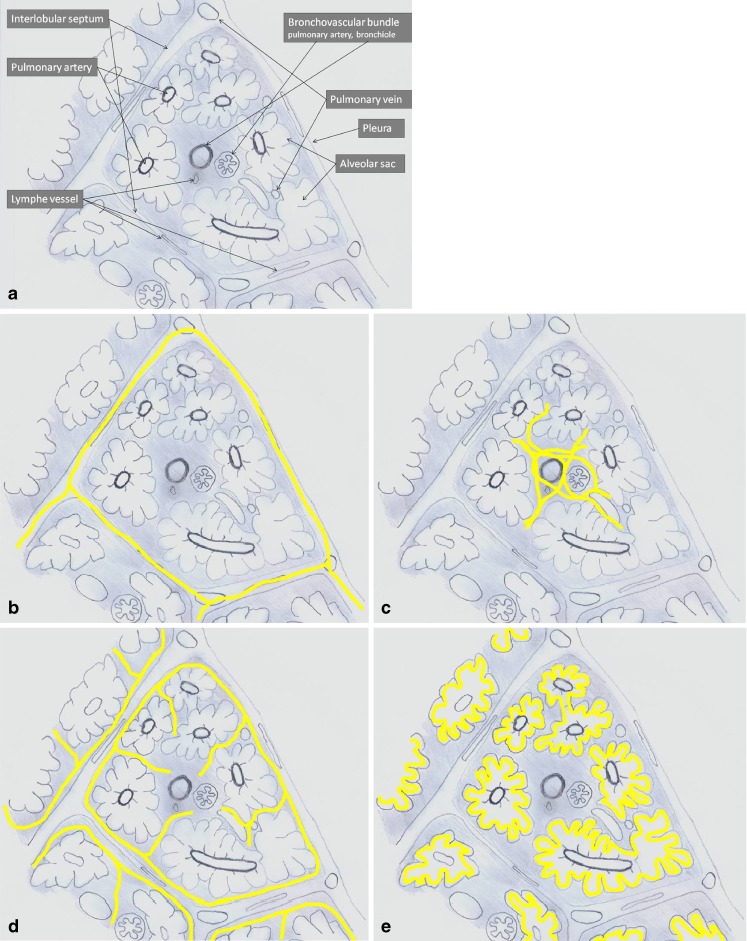
a Anatomy of the secondary pulmonary lobule. b–e The reticular pattern: b thickening of the interlobular septa; c thickening of the intralobular interstitium; d irregular areas of fibrosis; e periacinar pattern
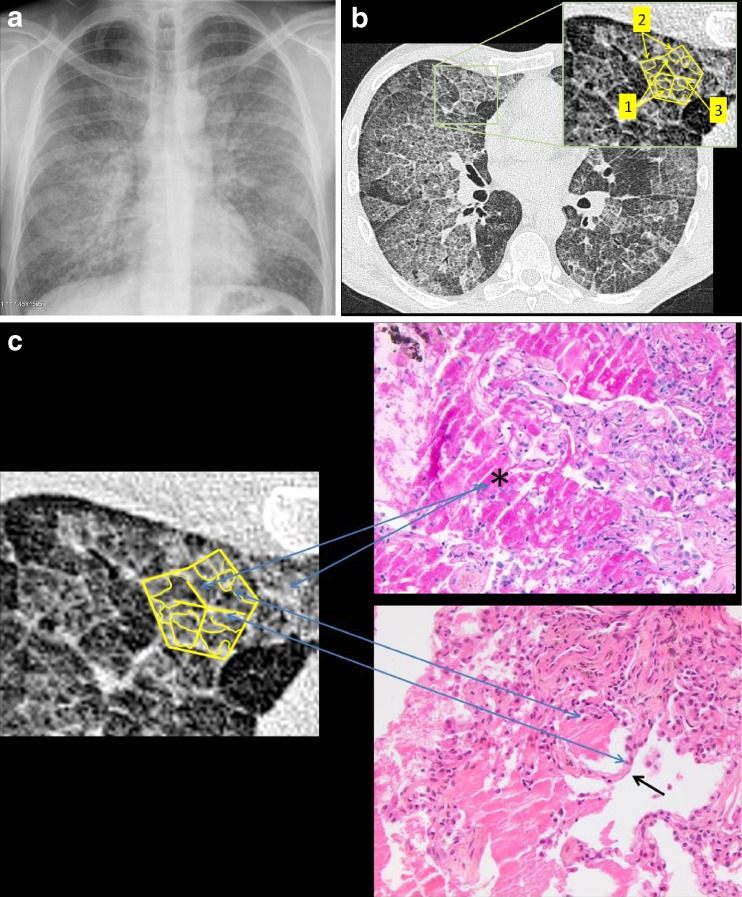
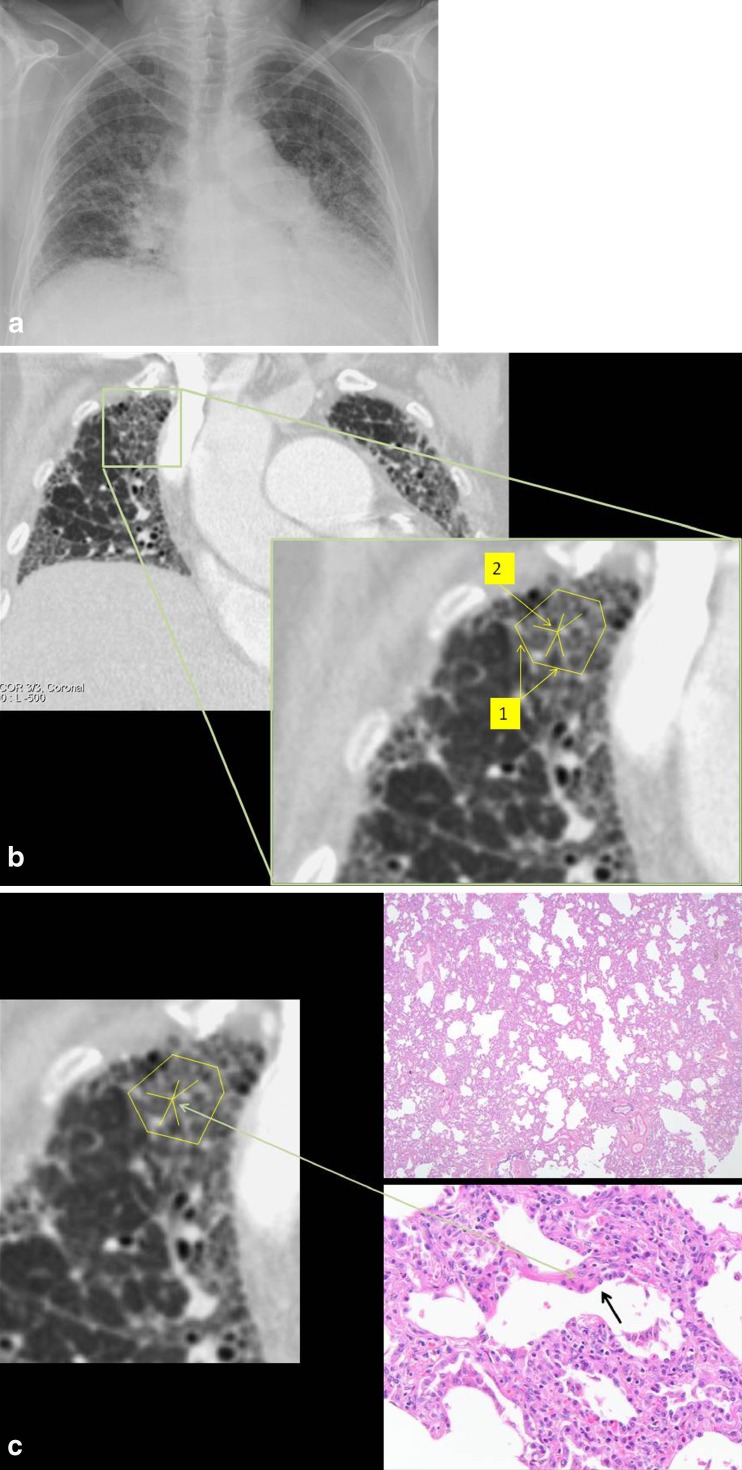
Alveolar proteinosis. a Chest radiograph showed a reticular pattern that was most pronounced in the central parts of the lungs. There was also a decrease in the lung translucency centrally in both lungs. Heart and central vessels were normal. There was no pleural effusion. b On CT, a patchy distribution of a crazy-paving pattern was visible. The lines corresponded to a deposition of material within the airspaces at the borders of the acini (1) in the secondary pulmonary lobules, but also along the interlobular (2) and intralobular septa (3): the periacinar pattern. c Radiological-histopathological correlation. Histopathological evaluation of a specimen out of the right lung showed amorphous eosinophilic material in the alveoli (*) positive on periodic acid Schiff (PAS) staining. This material corresponded to deficient surfactant. Filling of the alveoli (*) was responsible for the ground-glass appearance on CT. When the airspaces adjacent to the inter- and intralobular septa (black arrow) and to the alveolar walls filled, the periacinar pattern became visible
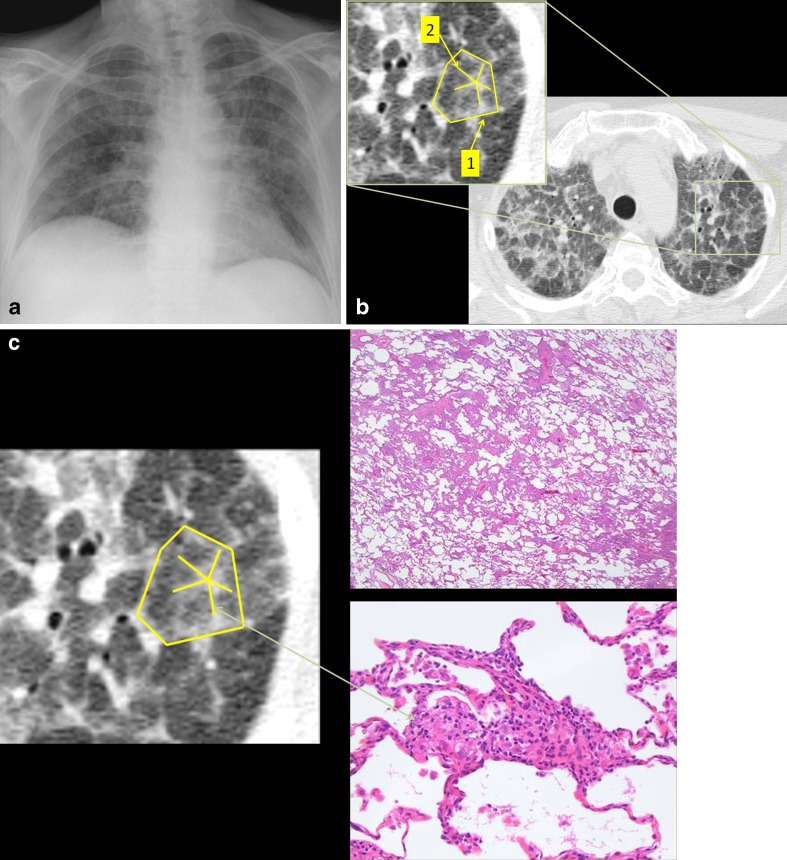
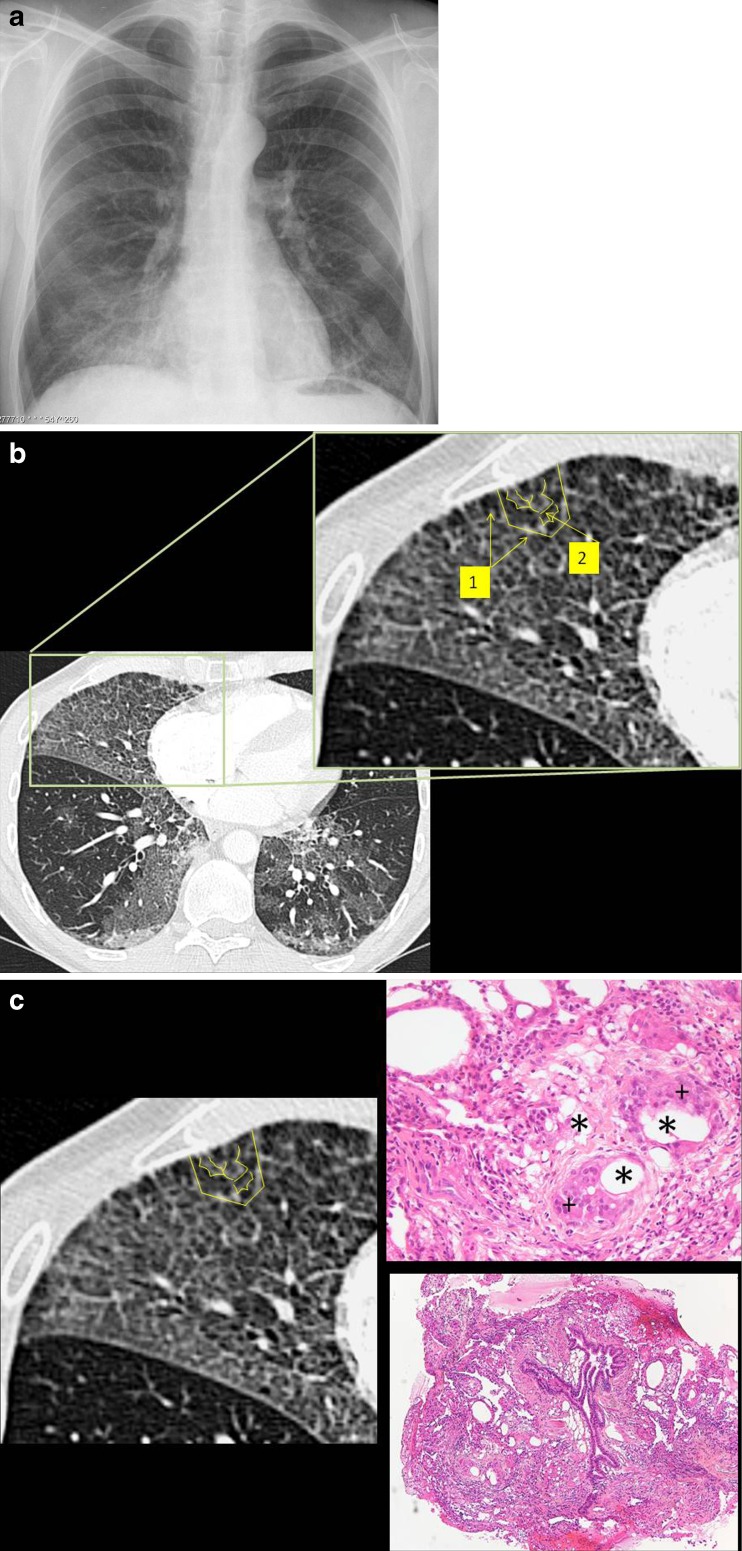
Hypersensitivity pneumonitis. a Chest radiograph showed patchy distribution of areas with increased lung density. There was also an increase in the linear pattern in both lungs. b On CT, a crazy-paving pattern was seen with a geographic distribution of ground-glass opacities with the superimposition of thickened inter- (1) and intralobular (2) septa. The findings were seen predominantly in the upper lung areas. c Radiological-histopathological correlation. Histology demonstrated interstitial pneumonia with lymphocytes, plasma cells and foamy macrophages in the interstitium. Epithelioid granulomas without caseation were also seen. There was no fibrosis. The alterations in the walls of the alveoli and the inflammation in the interstitium were visible as thickening of the inter- and intralobular lines
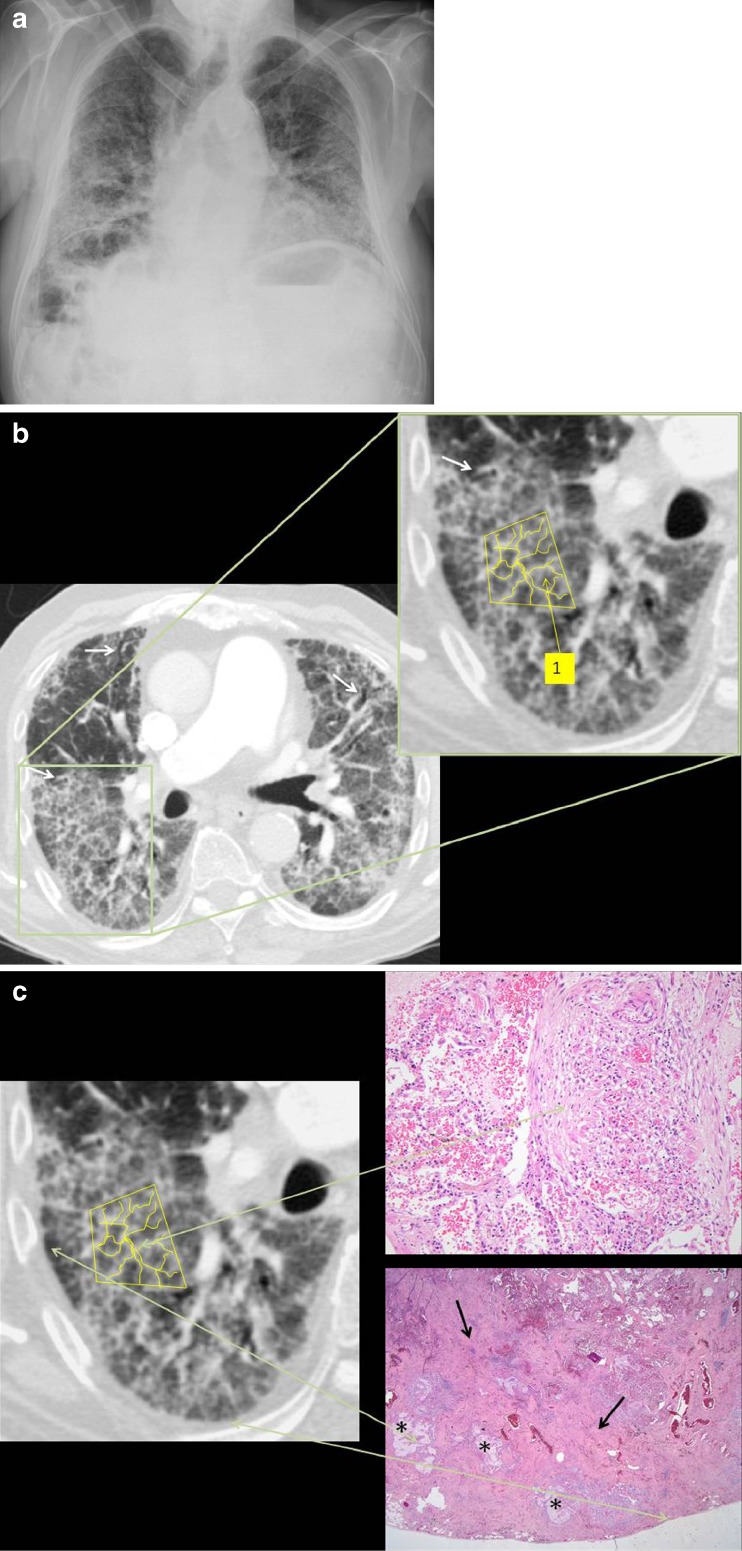
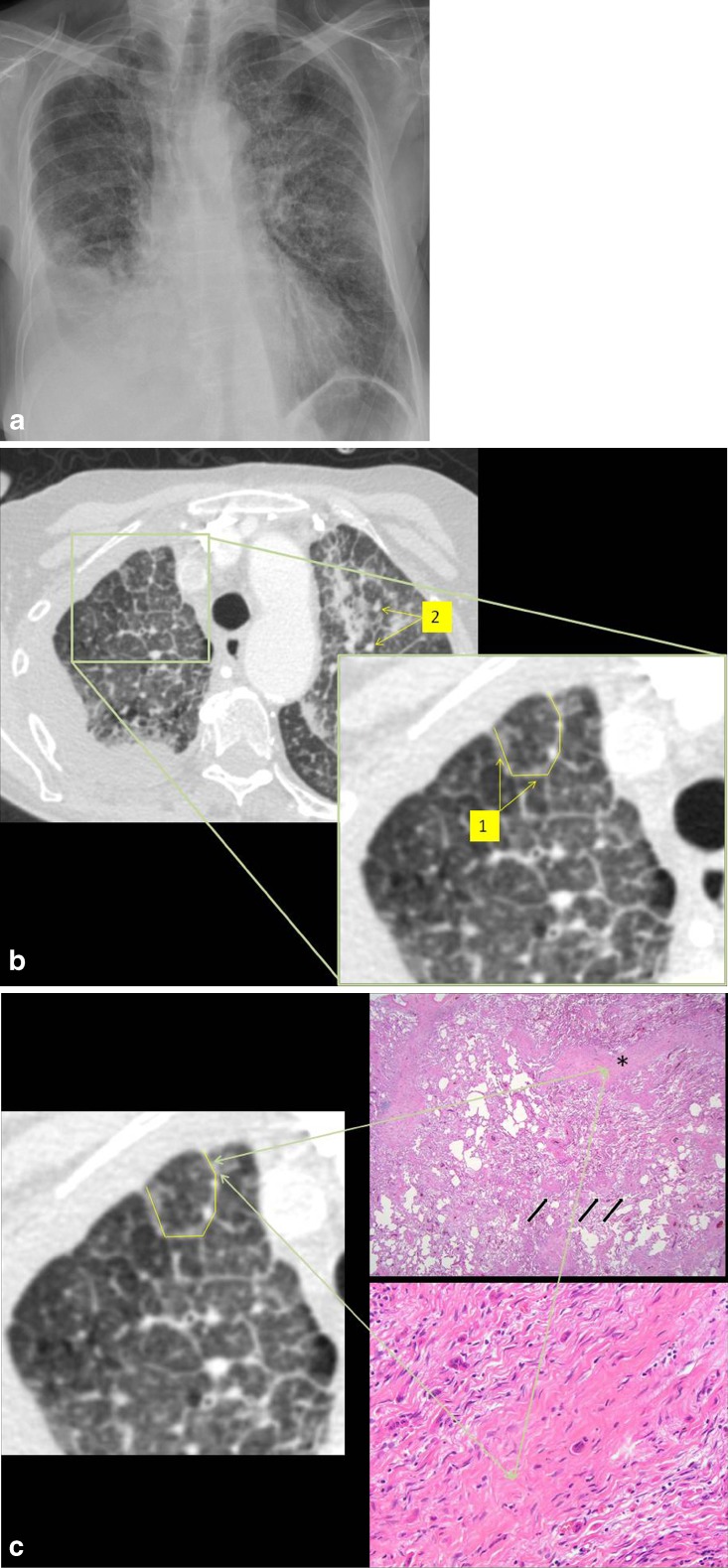
Usual interstitial pneumonia. a Chest radiograph showed patchy distribution of areas with consolidation and a fine reticular pattern, most pronounced in the periphery of both lungs. b A crazy-paving pattern was visible with scattered distribution. Superimposed on the ground-glass opacities a linear pattern with multiple small irregular lines was visible (intralobular fibrosis) (1). Traction bronchiectasis was seen in the periphery of both lungs (white arrow). c Radiological-histopathological correlation. On histology, thickening of the interstitium (arrow) with variable severity was seen, leaving some alveolar septa almost completely normal, whereas others were thickened. Fibrinous exudates, honeycombing (*) and mild inflammatory alveolitis were also present
Non-specific interstitial pneumonia. a Chest radiograph showed reticulation in the lung parenchyma, diffusely spread in both lungs, centrally and peripherally. b Chest CT showed a crazy-paving pattern especially at the periphery of both lungs. There was an increase in lung attenuation (ground-glass opacification) with a superimposition of a reticular pattern with thickening of the inter- (1) and intralobular (2) septa. c Radiological-histopathological correlation. Histological evaluation showed a homogeneous fibrotic thickening of the interstitium with inflammation. Macrophages were visible within the alveolar septa. Homogeneous interstitial inflammation was seen, corresponding to the diffuse ground-glass opacities, whereas fibrosis in the interstitium and alveolar septa (black arrow) was related to the superimposed linear pattern
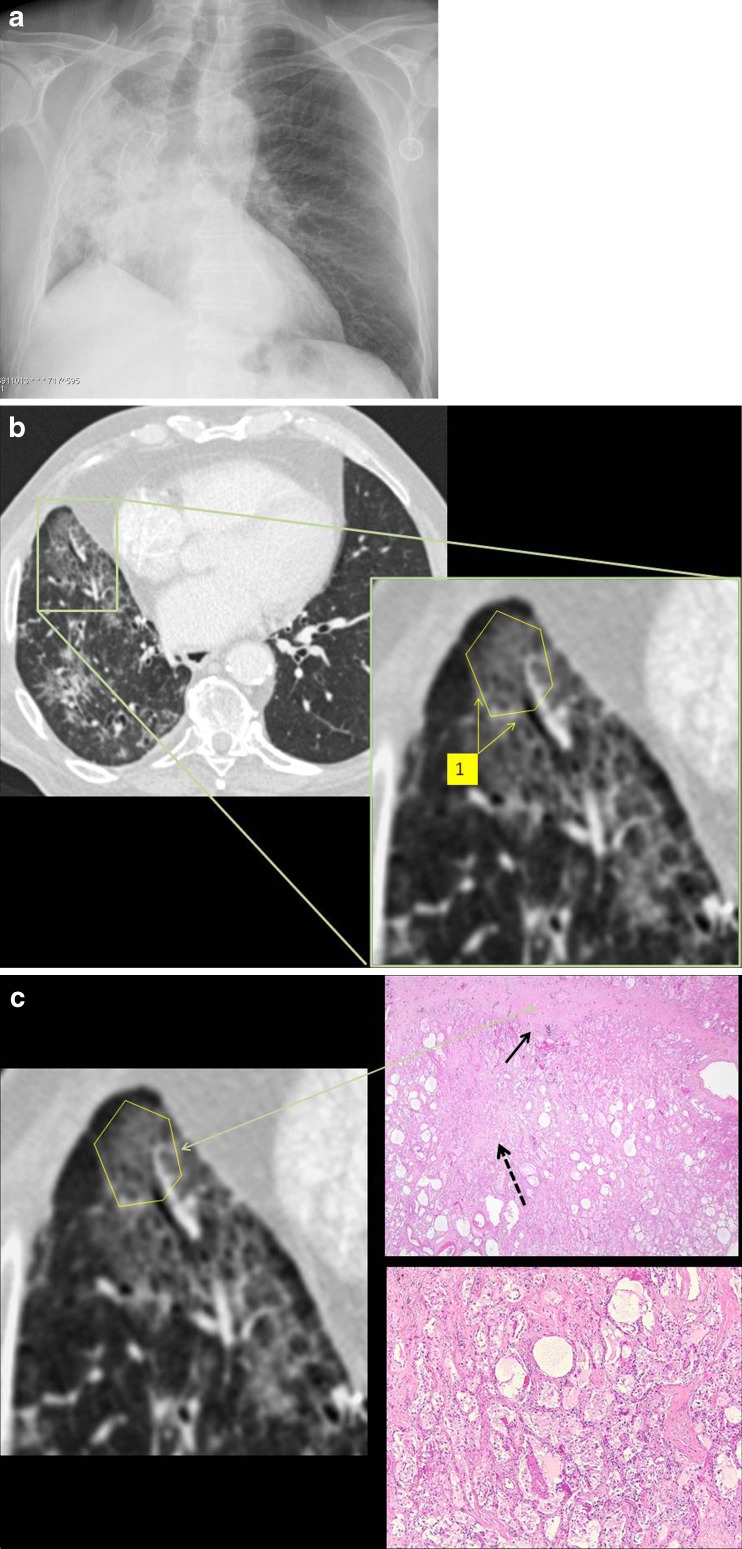
Radiation pneumonitis. a Chest radiograph showed an area of consolidation in the right lung with an air bronchogram. There was also loss of volume of the right lung. b CT showed the therapy response of the tumour. There was patchy distribution of a crazy-paving pattern with increased lung attenuation (ground-glass opacity) and thickening of the interlobular septa in the right lung (1). c Radiological-histopathological correlation. Histological examination after autopsy showed airspace filling with an exudate in combination with thickening of the interlobular septa (arrow), thickening of the interstitium surrounding the airspaces and also the presence of irregular fibrosis (dotted arrow). Alveolar spaces filled with an exudate of proteinaceous material were responsible for the ground-glass opacities on CT. The reticular pattern was due to congestion of capillaries and oedema of the interstitium
Exogenous lipid pneumonia. a Chest radiograph showed a decrease in lung translucency in the caudal region of the right lung with an air bronchogram. b Chest CT showed a crazy-paving pattern with areas of increased lung attenuation and with thickening of interlobular septa (1), even thickening of the intralobular interstitium (2). c Radiological-histopathological correlation. Histological examination showed alveoli filled with lipid particles (*), some ingested in macrophages (+) with the formation of lipid granulomas
Lymphangitic carcinomatosis. a Chest radiograph showed a pleural effusion in the right haemothorax. An increased linear pattern was seen in the left and right upper lung. b CT showed a diffuse crazy-paving pattern with areas of ground-glass attenuation and thickening of the interlobular septa (1). There were also some small nodular lesions visible mostly in the left upper lobe suggestive of pulmonary metastases (2). c Radiological-histopathological correlation. Histological examination of the autopsy specimen demonstrated thickening of the interlobular septa (*) due to fibrosis and the presence of tumour cells. There was also perivascular (arrow) thickening due to an expansion of lymphatic spaces by tumour cells. The histological reaction was that of diffuse alveolar damage and consisted of hyaline membranes in the alveolar ducts and respiratory bronchioles while the alveolar spaces fill with an exudate of proteinaceous material. This corresponded to the ground-glass opacities on CT. The reticular pattern was due to congestion of capillaries and oedema of the interstitium
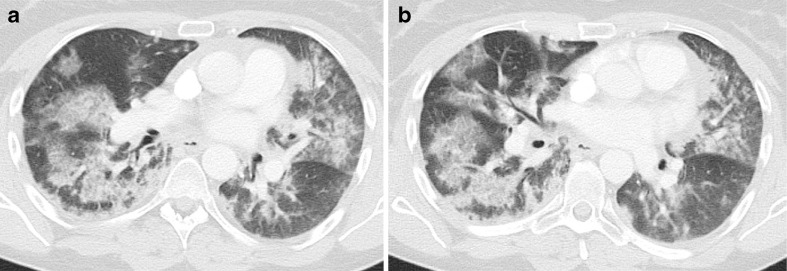
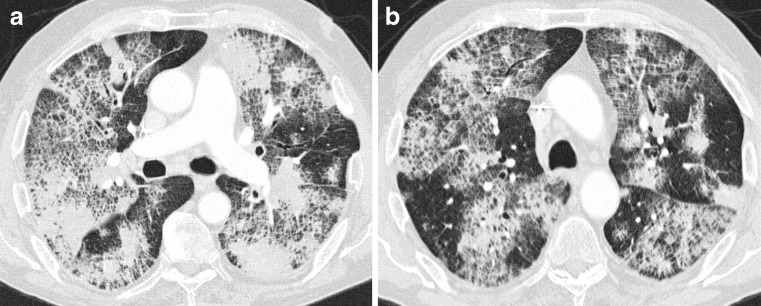
Pneumocystis jirovecii infection. CT showed a patchy distribution of areas with ground-glass opacification in both lungs, more pronounced in central parts, with a superimposition of a linear pattern
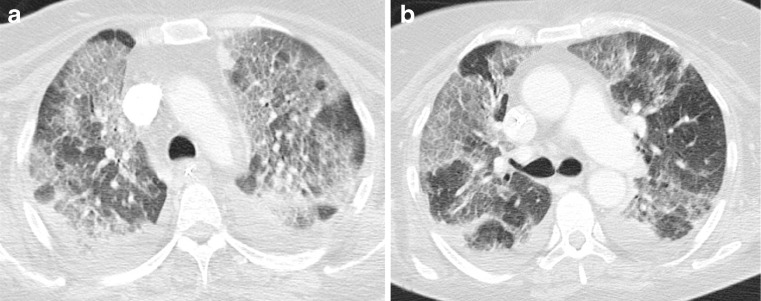
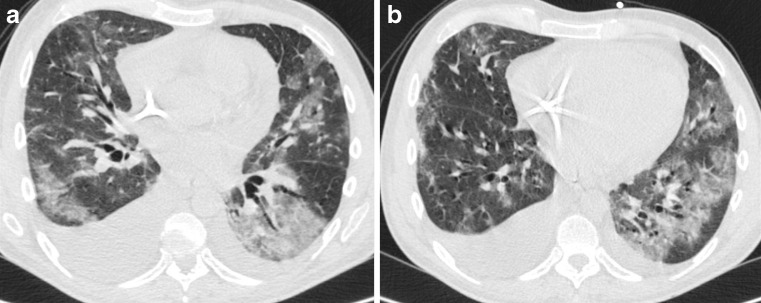
Acute respiratory distress syndrome. CT revealed bilateral areas with ground-glass attenuation superimposed with a reticular pattern. These lines corresponded to thickening of the interlobular septa, but also thickening of the intralobular interstitium
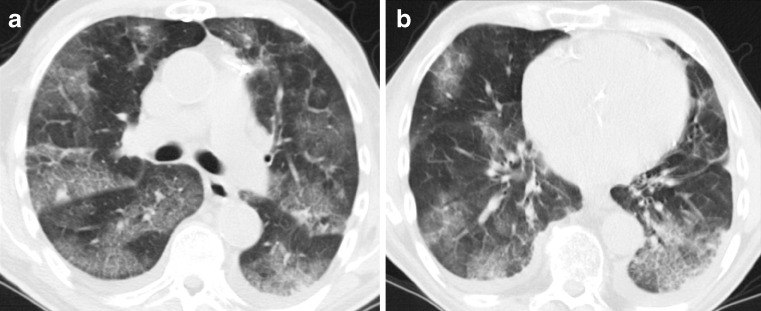
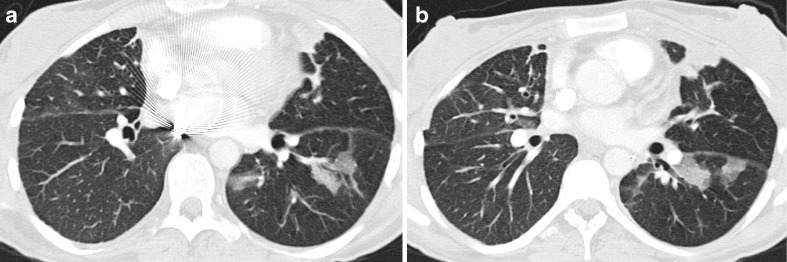
Pulmonary oedema. CT showed patchy distribution of areas with ground-glass opacification and a linear pattern. Most of the lines were thickened interlobular septa. Within the secondary pulmonary lobule, enlarged vascular structures with a spider configuration were seen. There were also some other intralobular lines
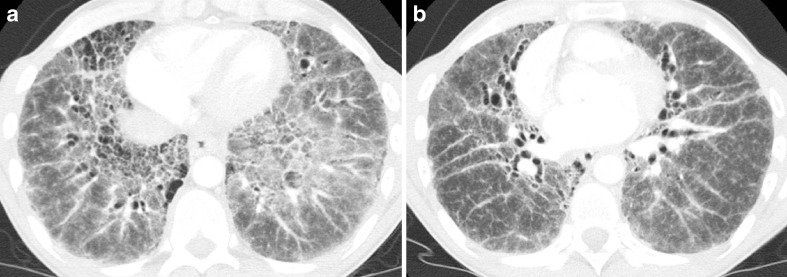
Sarcoidosis. CT showed a diffuse increase in lung attenuation (ground-glass attenuation) with the superimposition of an irregular reticular pattern: thickening of the interstitium and thickening of the peribronchovascular interstitium
Graft-versus-host disease. CT revealed multiple areas of ground-glass attenuation and consolidations. There was also a superimposition of multiple lines: thickened inter- and intralobular septa and intralobular fibrosis
Organising pneumonia. CT showed patchy distribution of areas of ground-glass opacification with the superimposition of thickened interlobular septa
Bronchioloalveolar carcinoma. CT showed patchy distribution of areas with ground-glass opacification and areas with consolidation. Superimposed on these areas there is a reticular pattern corresponding to the thickening of the interstitium
References
-
- Verschakelen JA, Wever W. Computed tomography of the lung. A pattern approach. Heidelberg: Springer; 2007.
LinkOut - more resources
Full Text Sources