

Imaging the spine in arthritis-a pictorial review
- PMID: 22347946
- PMCID: PMC3259357
- DOI: 10.1007/s13244-010-0061-4
Imaging the spine in arthritis-a pictorial review
Abstract
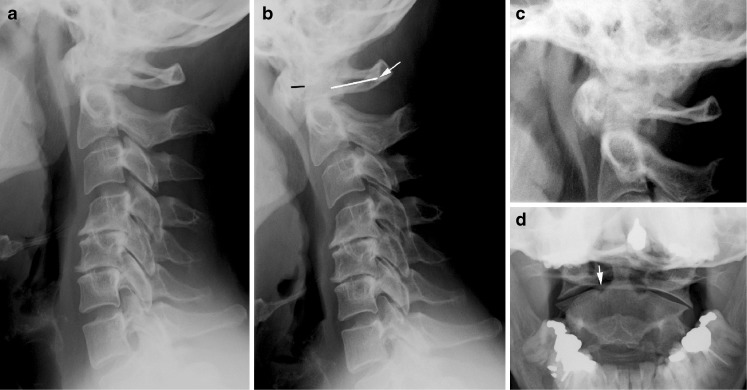
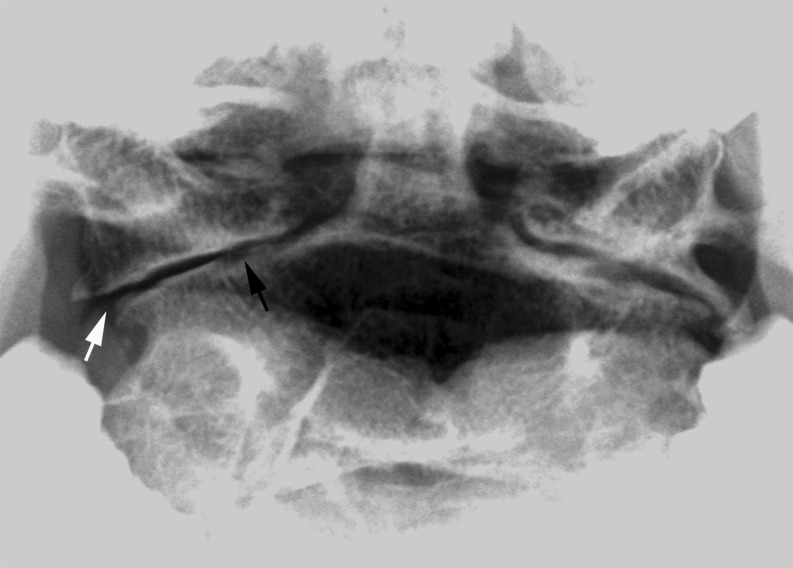
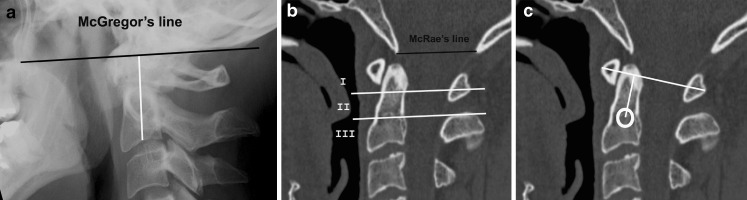
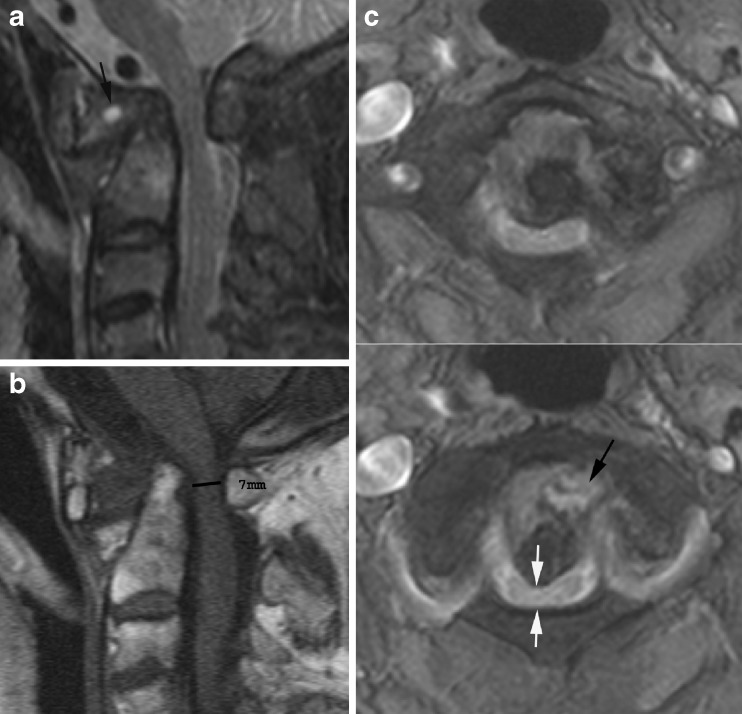
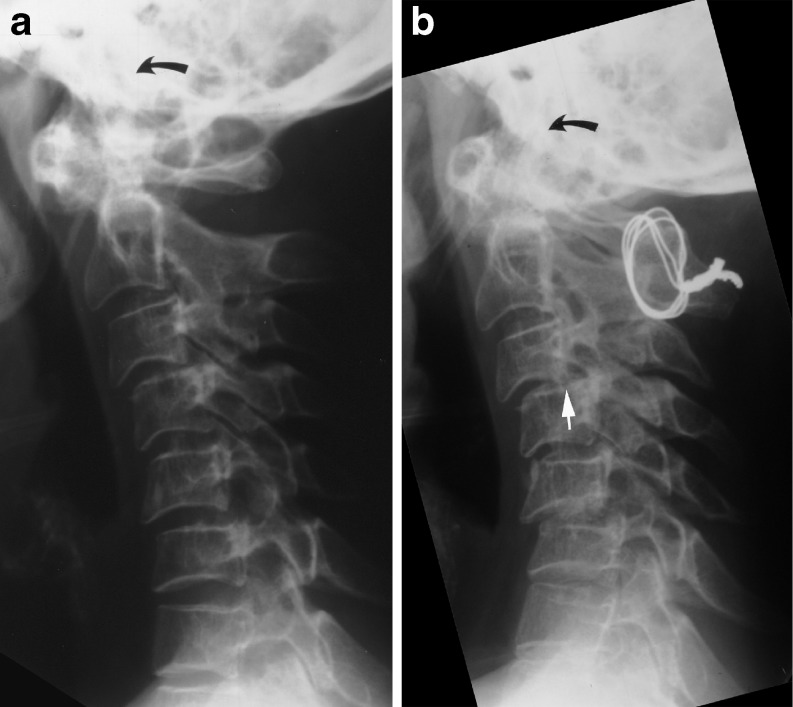
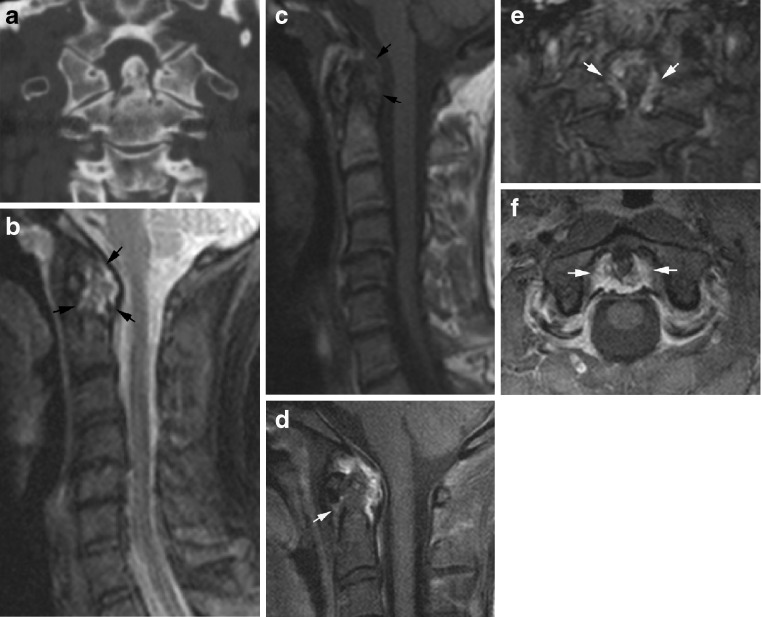
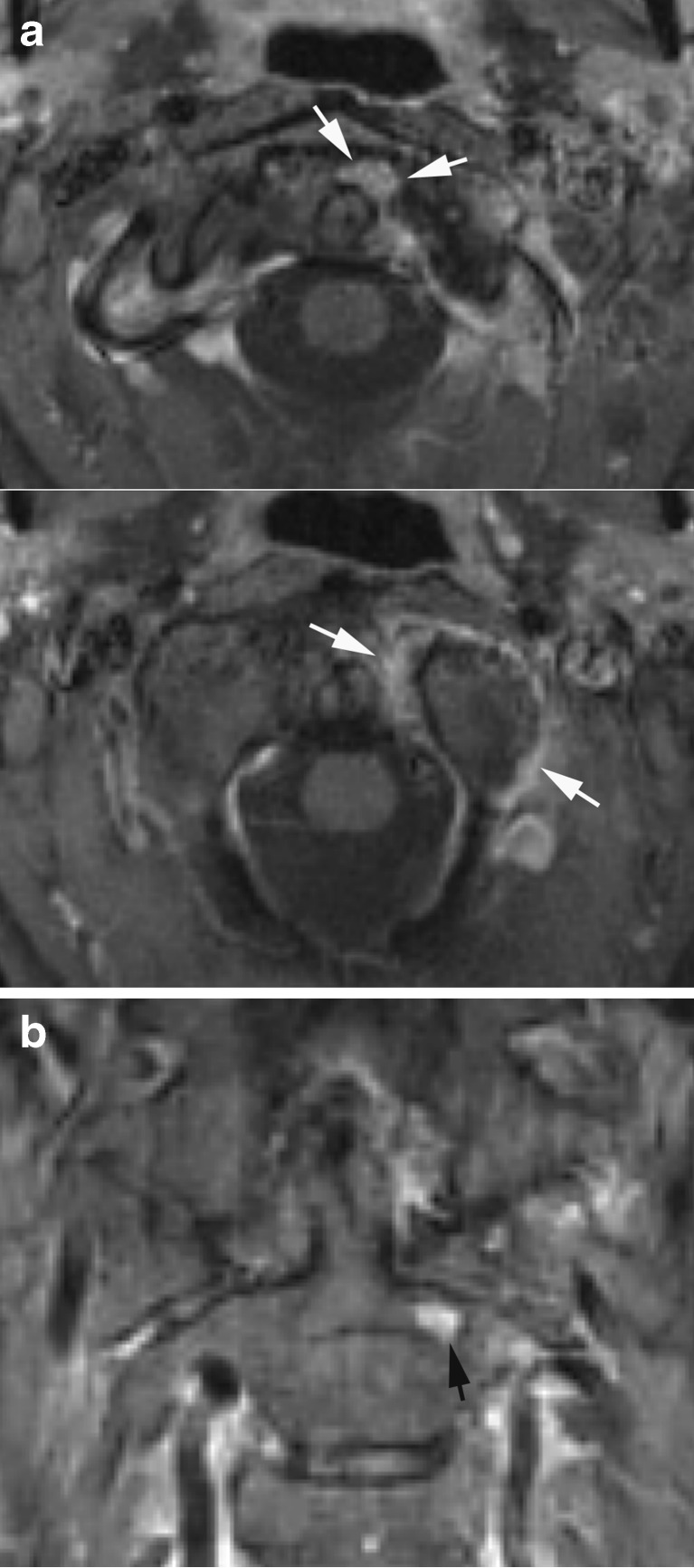
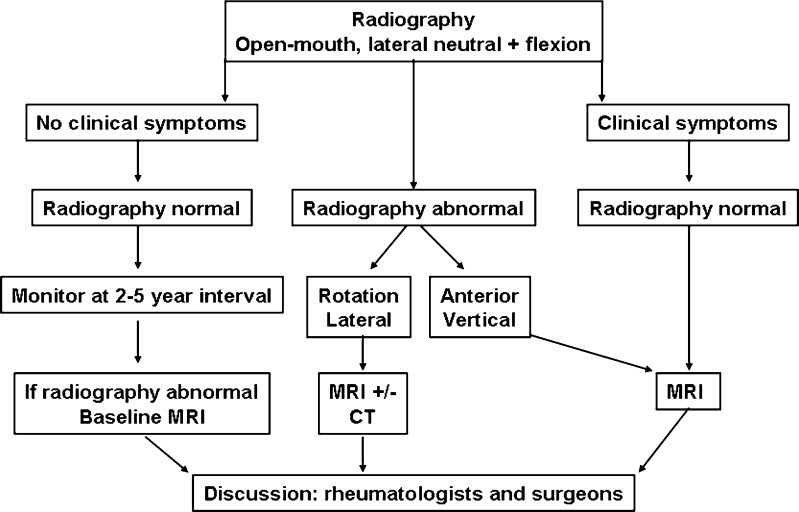
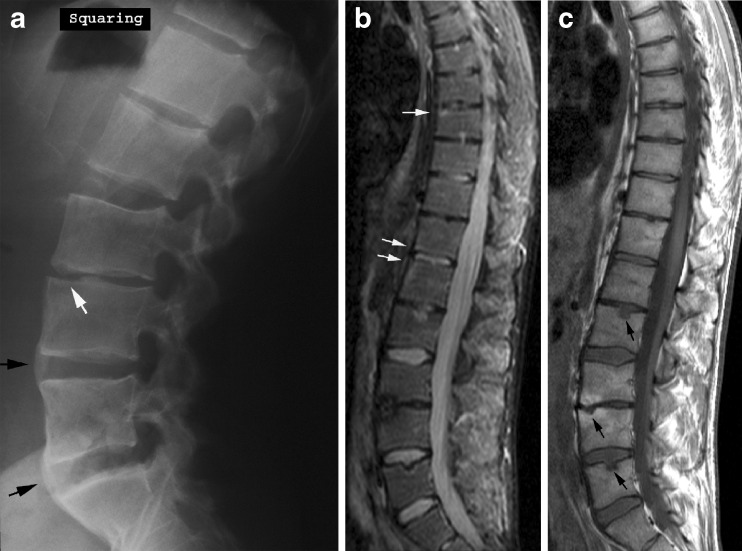
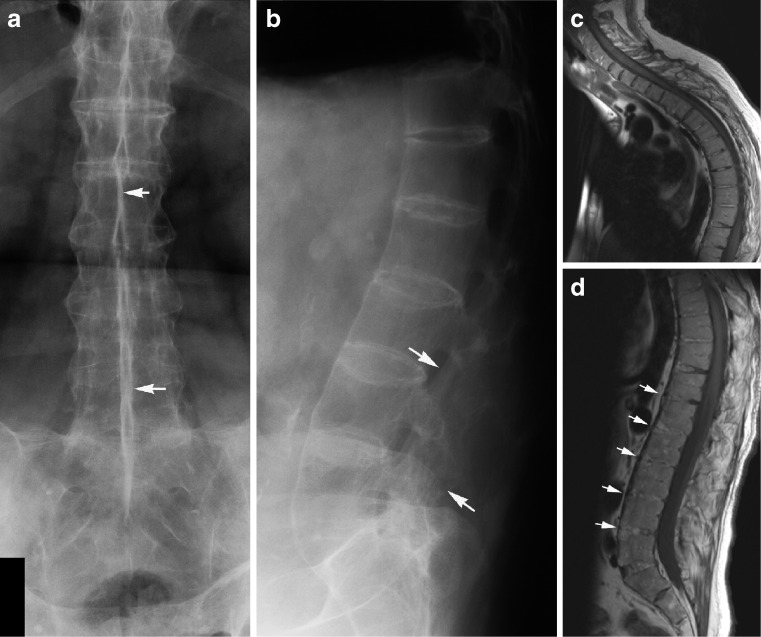
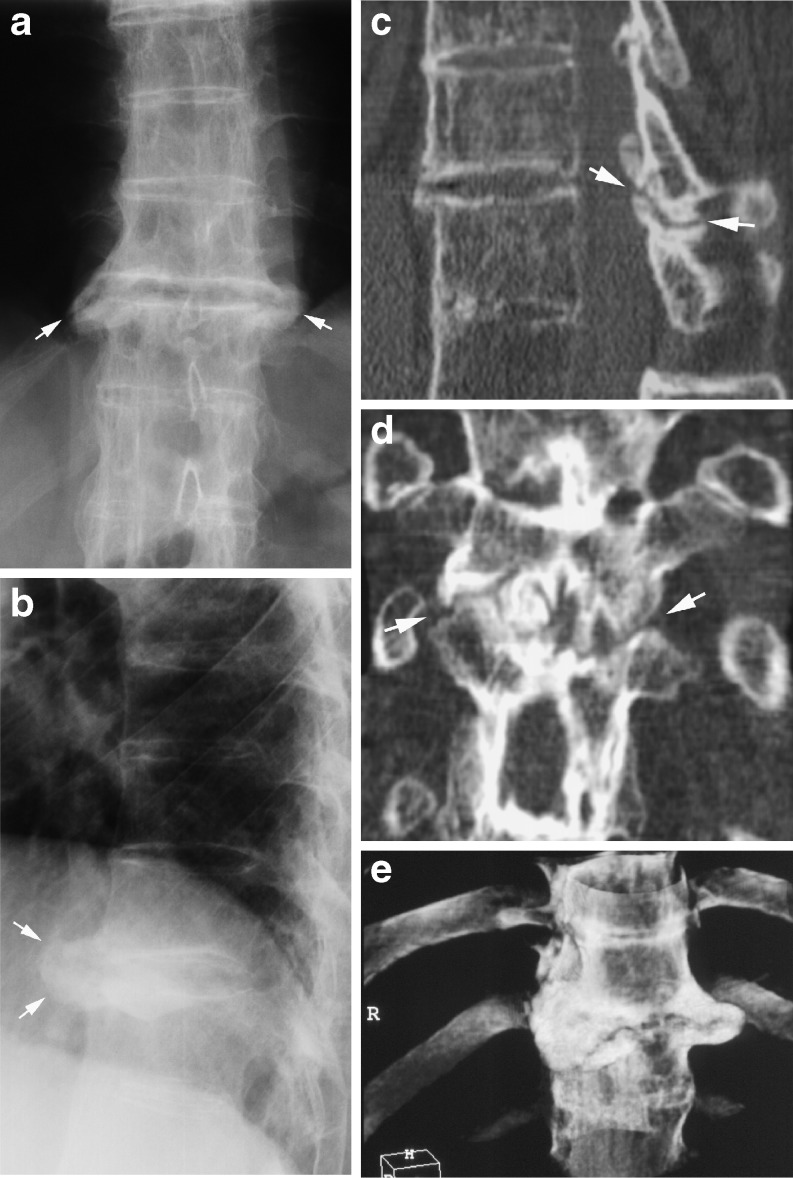
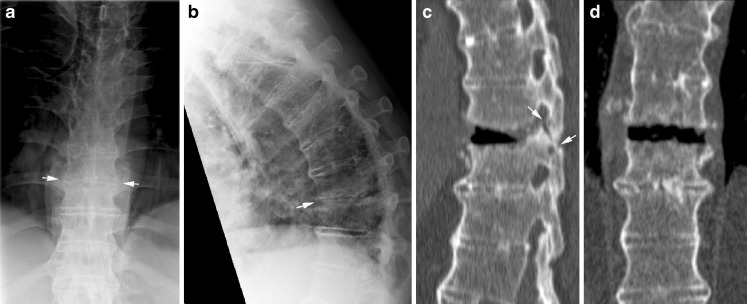
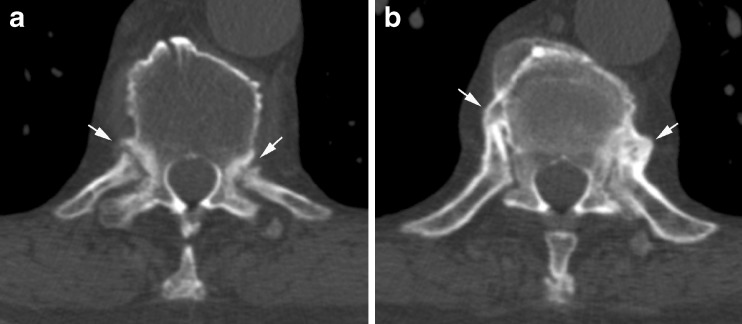
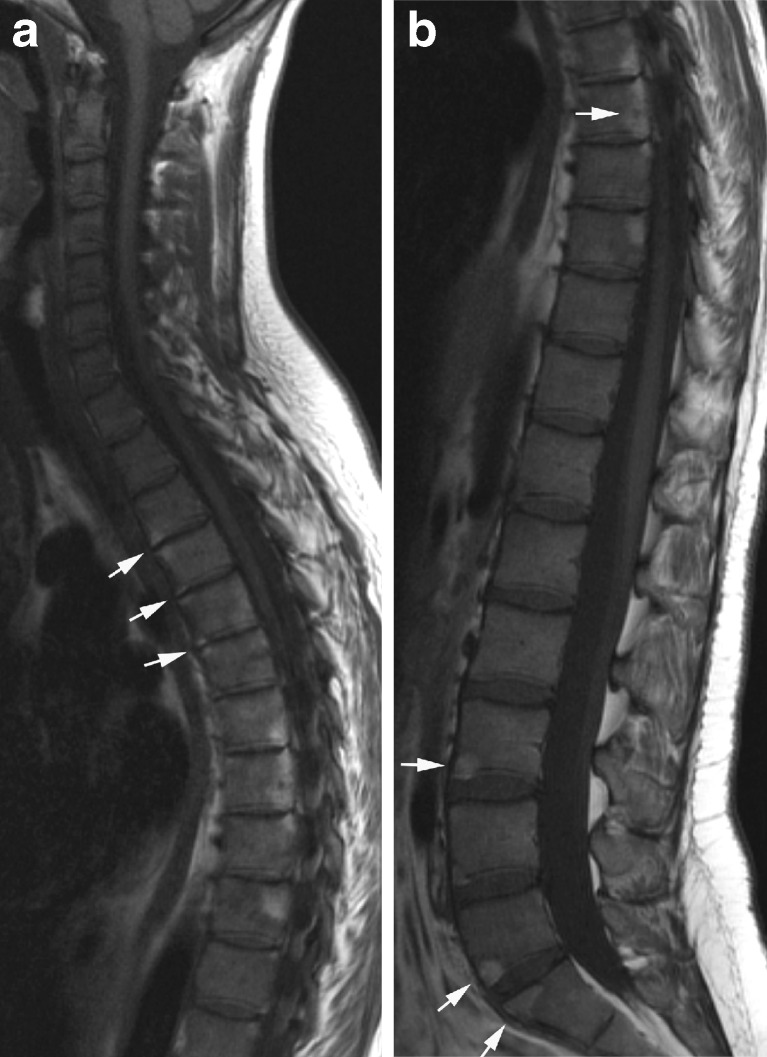
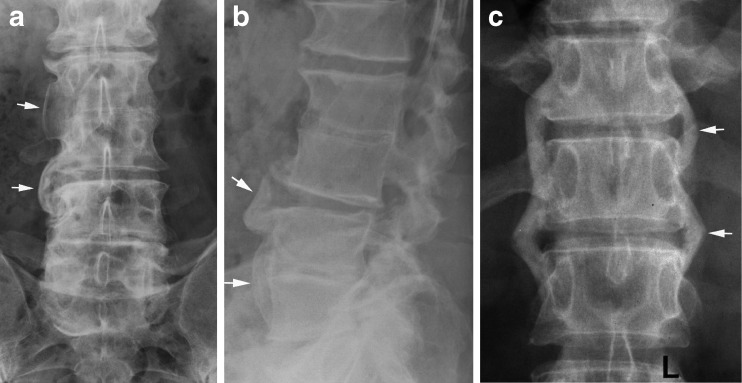
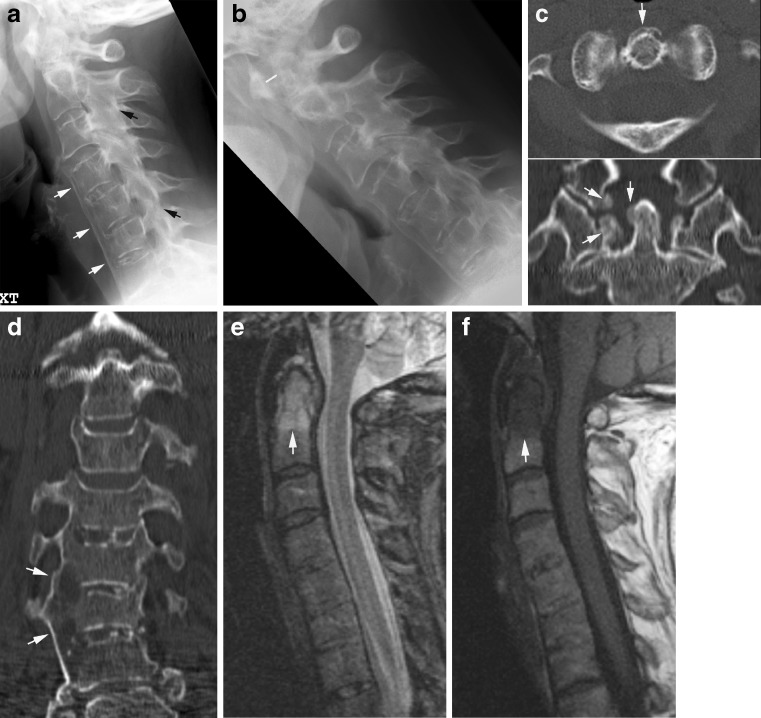
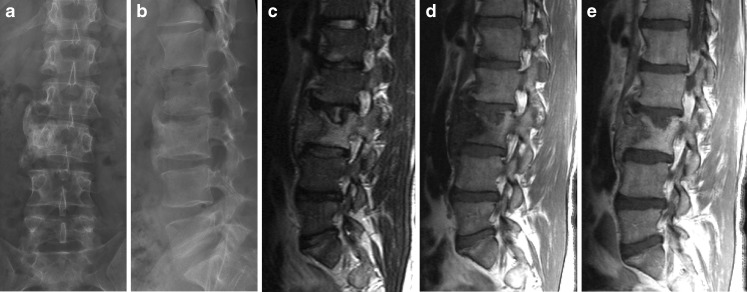
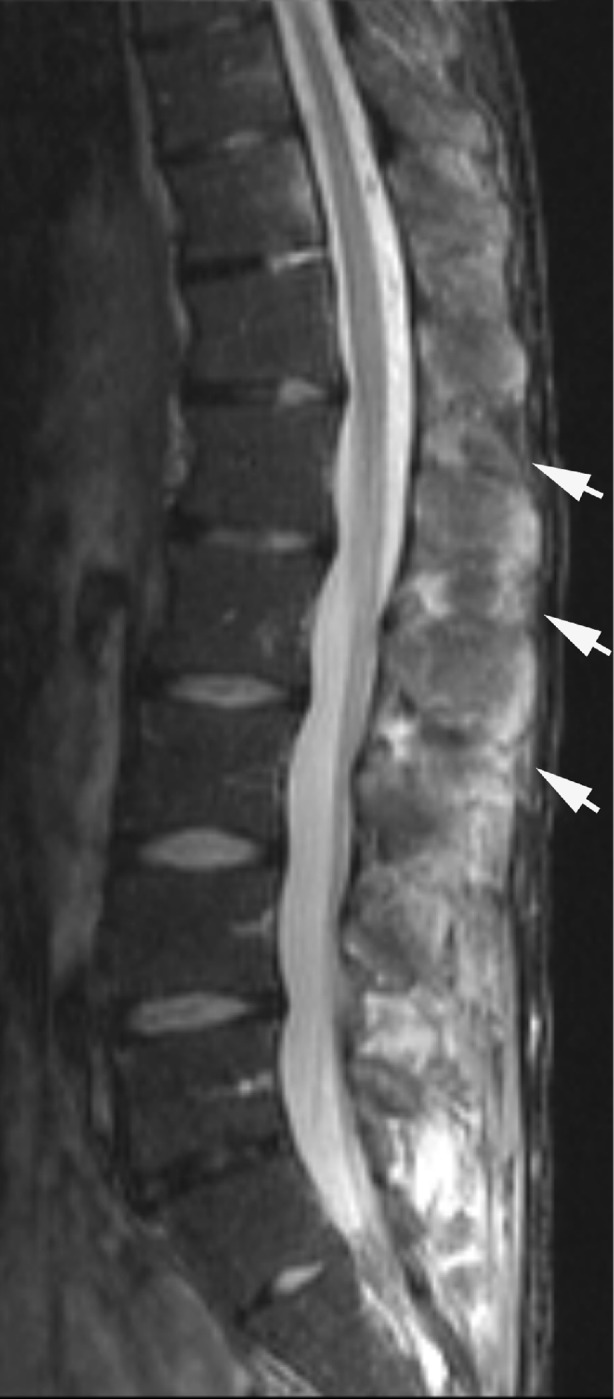
Spinal involvement is frequent in rheumatoid arthritis (RA) and seronegative spondyloarthritides (SpA), and its diagnosis is important. Thus, MRI and CT are increasingly used, although radiography is the recommended initial examination. The purpose of this review is to present the typical radiographic features of spinal changes in RA and SpA in addition to the advantages of MRI and CT, respectively. RA changes are usually located in the cervical spine and can result in serious joint instability. Subluxation is diagnosed by radiography, but supplementary MRI and/or CT is always indicated to visualise the spinal cord and canal in patients with vertical subluxation, neck pain and/or neurological symptoms. SpA may involve all parts of the spine. Ankylosing spondylitis is the most frequent form of SpA and has rather characteristic radiographic features. In early stages it is characterised by vertebral squaring and condensation of vertebral corners, in later stages by slim ossifications between vertebral bodies, vertebral fusion, arthritis/ankylosis of apophyseal joints and ligamentous ossification causing spinal stiffness. The imaging features of the other forms of SpA can vary, but voluminous paravertebral ossifications often occur in psoriatic SpA. MRI can detect signs of active inflammation as well as chronic structural changes; CT is valuable for detecting fracture.
Figures



References
-
- Kim DH, Hilibrand AS. Rheumatoid arthritis in the cervical spine. J Am Acad Orthop Surg. 2005;13(7):463–474. - PubMed
-
- Riew KD, Hilibrand AS, Palumbo MA, Sethi N, Bohlman HH. Diagnosing basilar invagination in the rheumatoid patient. The reliability of radiographic criteria. J Bone Joint Surg Am. 2001;83(2):194–200. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials