

doi: 10.1007/s13244-011-0089-0.
Epub 2011 Apr 14.
Common primary tumours of the abdomen and pelvis and their patterns of tumour spread as seen on multi-detector computed tomography
- PMID: 22347948
- PMCID: PMC3259344
- DOI: 10.1007/s13244-011-0089-0
Item in Clipboard
Common primary tumours of the abdomen and pelvis and their patterns of tumour spread as seen on multi-detector computed tomography
Insights Imaging.
2011 Jun.
Abstract
BACKGROUND: Multidetector computed tomography (MDCT) has become the main investigation of choice for staging of many cancers. AIM: The purpose of this pictorial review is to discuss the imaging appearances on CT of some of the more common cancers arising within the abdomen and pelvis and to describe their typical sites of local, nodal and haematogenous tumour spread. METHODS: Cancers arising from the stomach, pancreas, colon, kidney, ovary and prostate will be reviewed. RESULTS: Awareness of the characteristic sites of tumour spread is important to allow accurate identification of all sites of disease. CONCLUSION: This will clearly have an impact on both patient management and prognosis.
Figures

Gastric adenocarcinoma: axial contrast-enhanced CT (CECT) showing tumour arising from the lesser curvature of the stomach (asterisk) associated with enlarged regional gastrohepatic nodes (arrows)
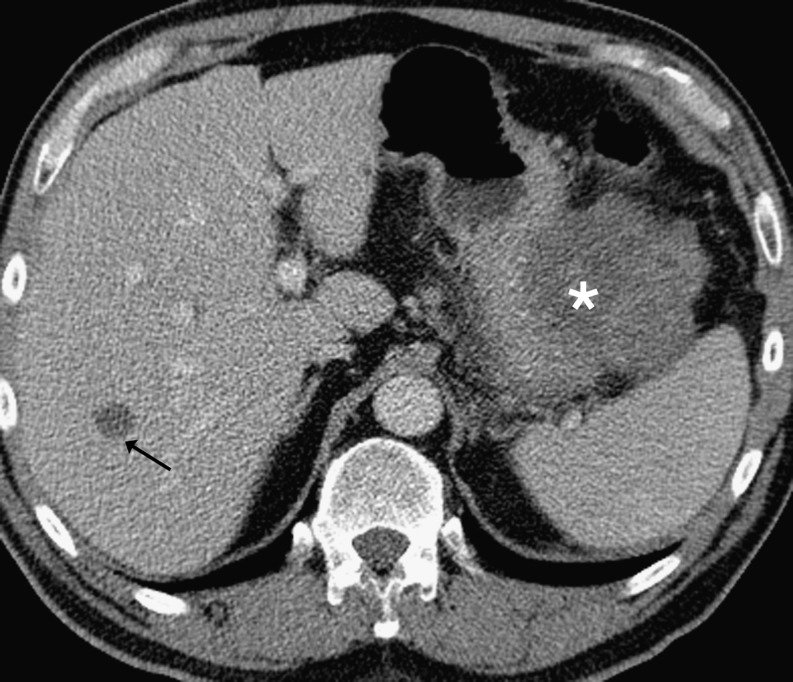
Gastrointestinal stromal tumour (GIST): axial CECT showing typical large low attenuation exophytic tumour (asterisk) arising from the greater curvature of the stomach associated with liver metastasis (arrow). Note there are no significantly enlarged regional nodes
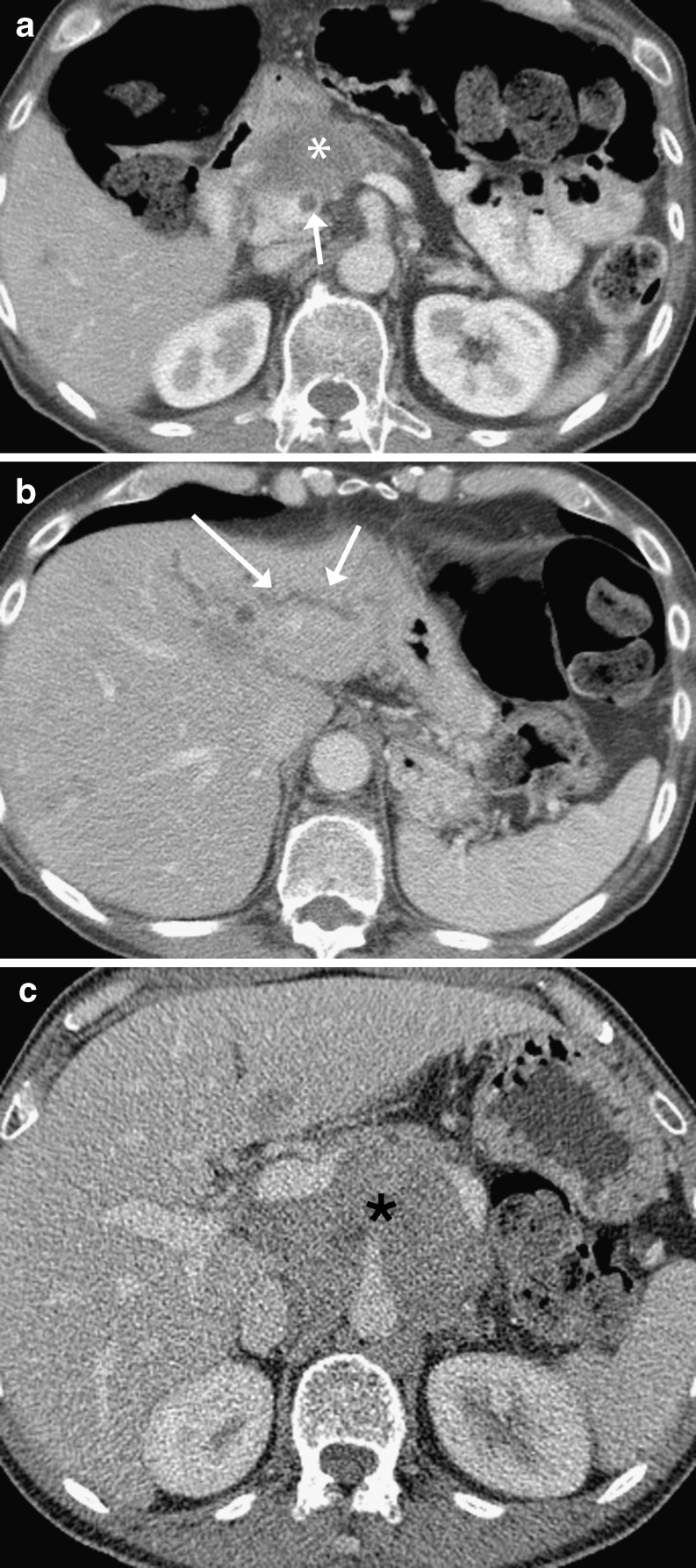
Pancreatic adenocarcinoma: a axial CECT showing an example of a tumour arising in the head of the pancreas (asterisk) with invasion into the duodenum. There is a focal thrombus in the portal vein (arrow); b axial CECT in same patient as (a); there is associated intra- (arrows) and extrahepatic (not shown) bile duct dilatation; c axial CECT showing a large bulky tumour in a different patient arising in the body of the pancreas (asterisk) encasing the origin of the celiac axis
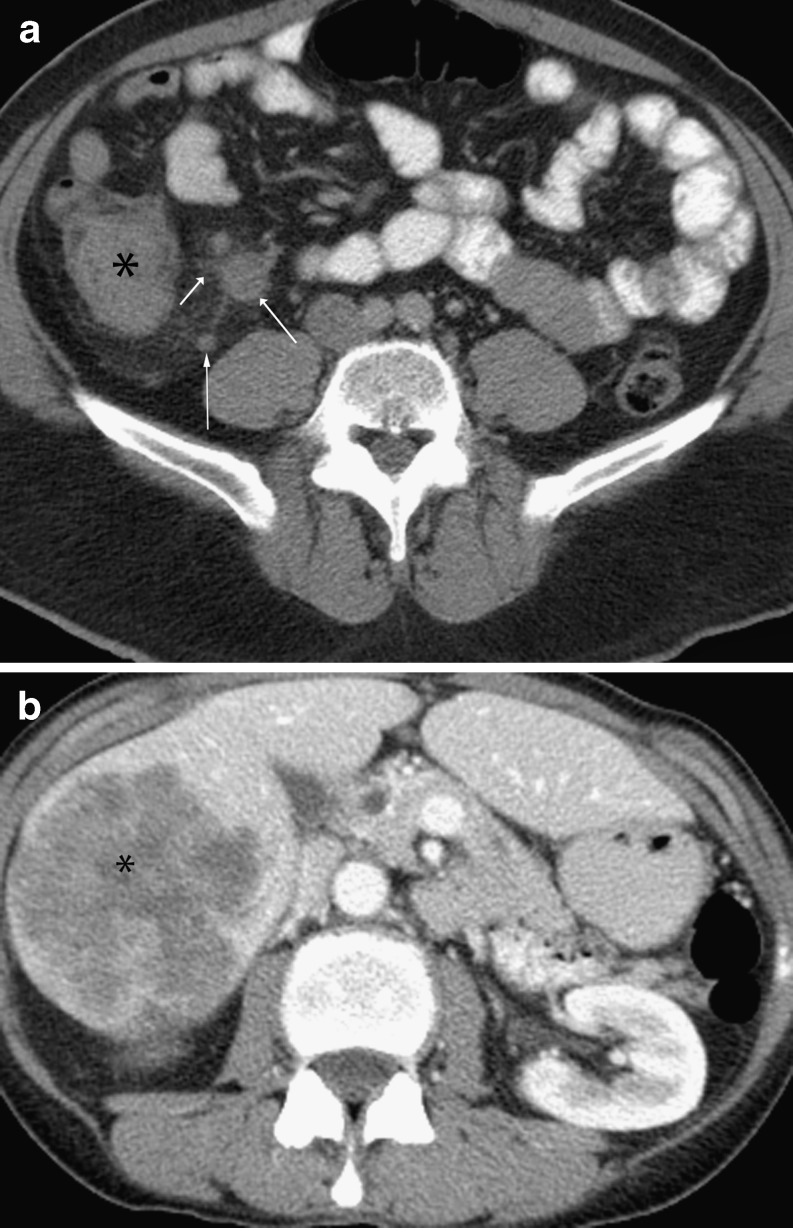
Colonic adenocarcinoma: a axial non-contrast-enhanced CT showing tumour (asterisk) in the ascending colon with enlarged ileocolic nodes (arrows); b axial contrast-enhanced CT shows a large liver metastasis (asterisk)

Rectal adenocarcinoma: coronal reformat CECT showing a bulky rectal tumour (asterisk) with enlarged right internal iliac nodes (double asterisk) and left paraaortic node (arrow)

Pseudomyxoma peritoneii: axial CECT showing mucinous ascites exerting mass effect (scalloping) on the solid organs; primary was of gastrointestinal tract origin
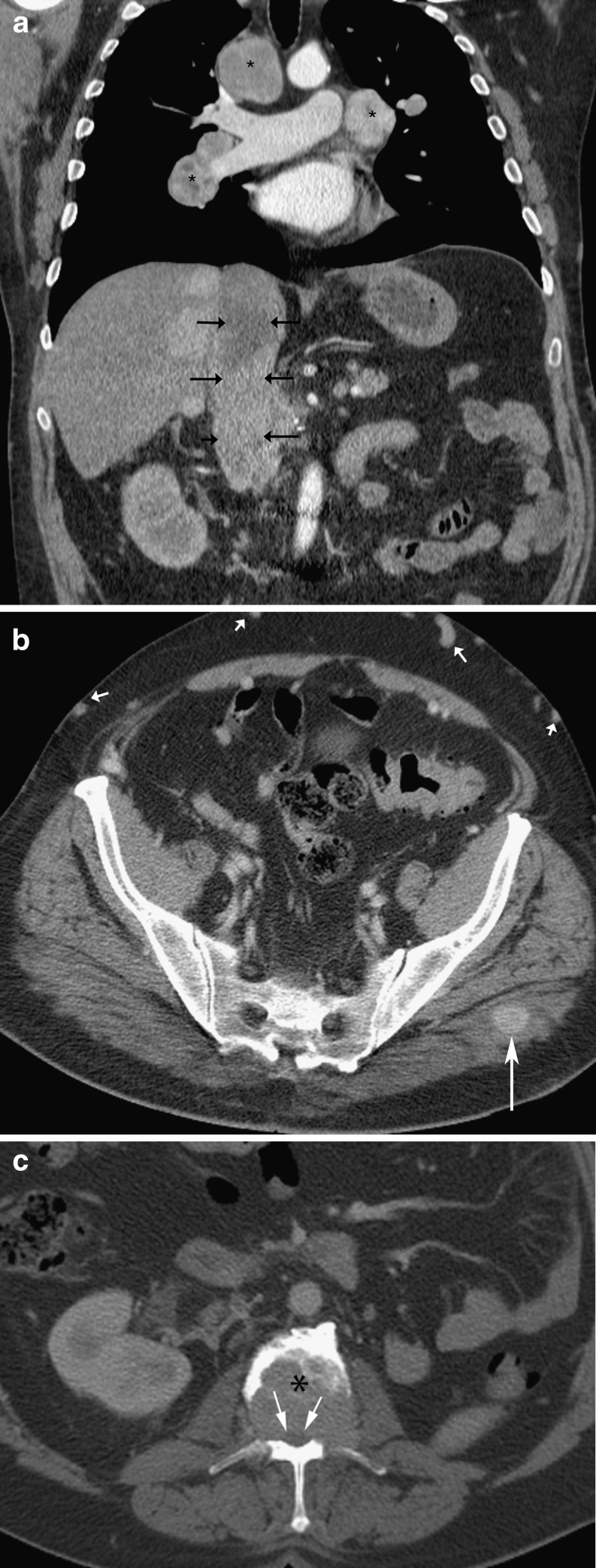
Metastatic renal cell carcinoma: a coronal reformat CECT showing the inferior vena cava (IVC) greatly expanded by tumour thrombus (arrows) with associated enlarged mediastinal nodes (asterisks). The primary renal tumour has been excised; b axial CECT showing enhancing lesion in the left gluteus maximus muscle in the same patient, which increased in size on interval CT studies, in keeping with a metastatic deposit; note the numerous venous collaterals in the anterior abdomen (short arrows) due to the IVC thrombus; c axial CECT shows a large lytic deposit in the lumbar spine (asterisk) in the same patient causing compromise of the spinal canal and cord (arrows)

Ovarian carcinoma: coronal reformat CECT showing a large solid/cystic adnexal mass arising from the pelvis (asterisk), with large-volume para-aortic adenopathy (double asterisk), ascites and small peritoneal deposits (arrows). Although para-aortic nodal involvement is seen in metastatic ovarian carcinoma, the large volume is rather unusual; b sagittal reformat CECT showing subcapsular deposits over the liver in a different patient (arrows); c axial CECT in the same patient as (b) showing a thick omental cake (arrows); d axial CECT in the same patient as (b) showing multiple enlarged (short axis diameter >5 mm) cardiophrenic nodes (arrows)
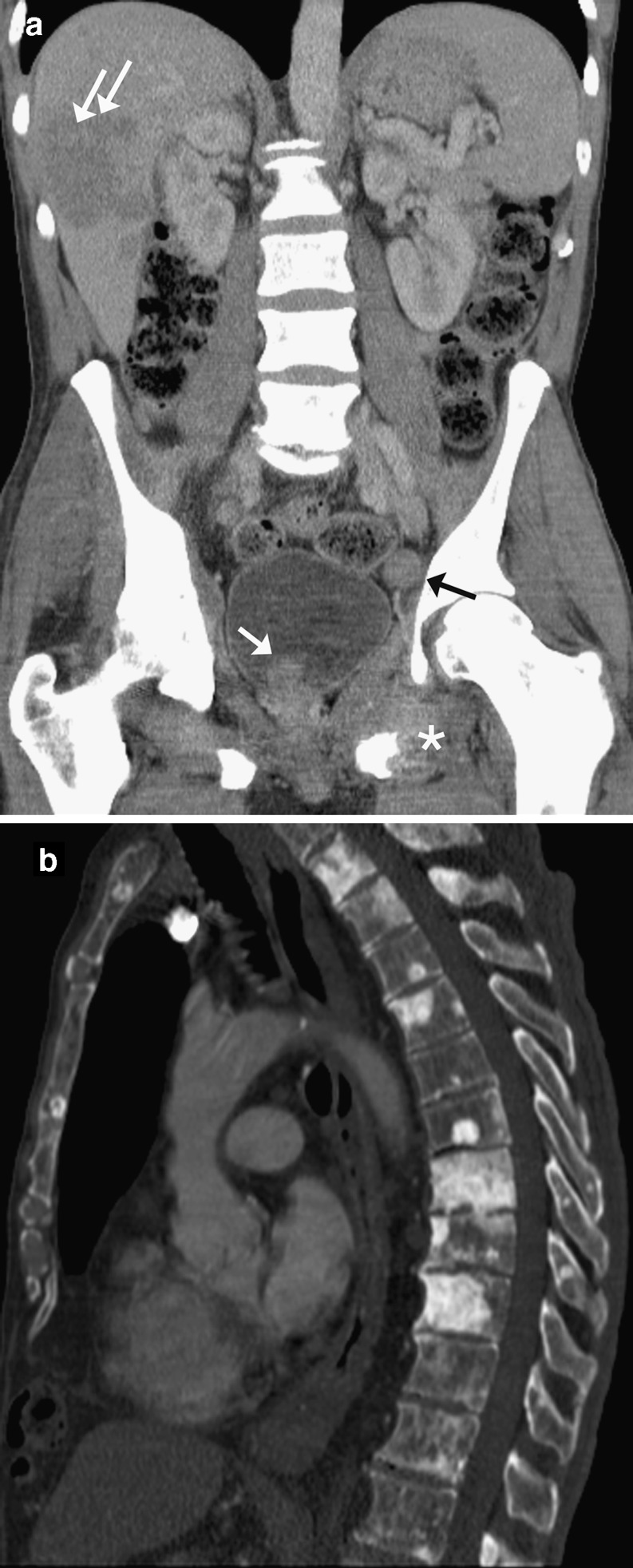
Prostate carcinoma: a coronal reformat CECT showing irregular enlarged prostate tumour (white arrow) extending into the bladder with enlarged left pelvic side wall node (black arrow), liver metastases (double arrows) and lesion in the left pubic ramus with large soft tissue component (*). Note the bones are sclerotic in keeping with diffuse bony metastases; b sagittal reformat CECT in a different patient on bone windows, showing multiple sclerotic metastases in the thoracolumbar spine
References
-
- Rossi M, Broglia L, Graziano P, Maccioni F, Bezzi M, Masciangelo R, Rossi P. Local invasion of gastric cancer: CT findings and pathologic correlation using 5-mm incremental scanning, hypotonia, and water filling. AJR Am J Roentgenol. 1999;172(2):383–388. - PubMed
-
- Chourmouzi D, Sinakos E, Papalavrentios L, Akriviadis E, Drevelegas A. Gastrointestinal stromal tumors: a pictorial review. J Gastrointestin Liver Dis. 2009;18(3):379–383. - PubMed
LinkOut - more resources
Full Text Sources