

CT imaging of blunt chest trauma
- PMID: 22347953
- PMCID: PMC3259405
- DOI: 10.1007/s13244-011-0072-9
CT imaging of blunt chest trauma
Abstract
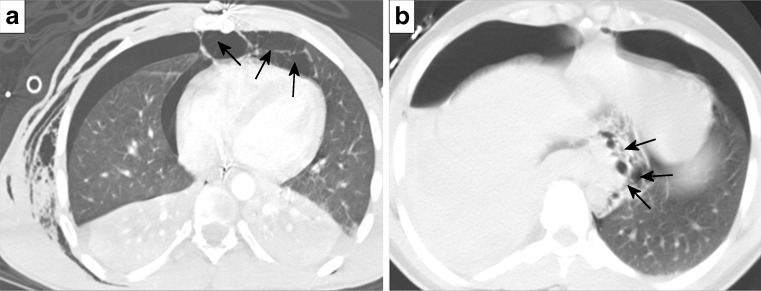
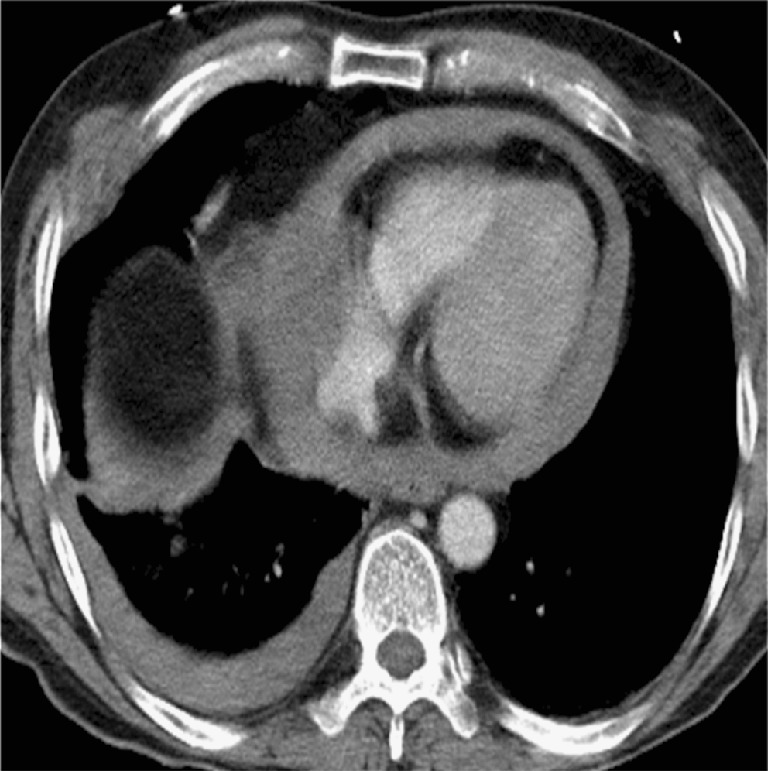
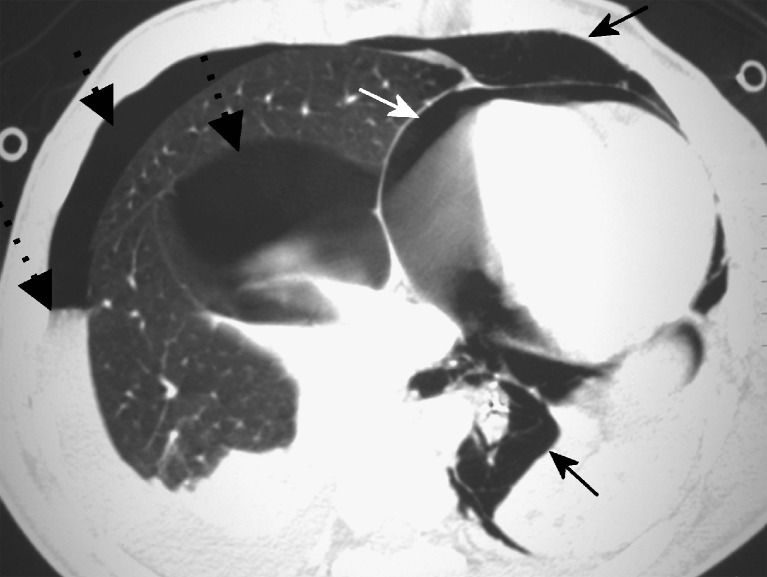
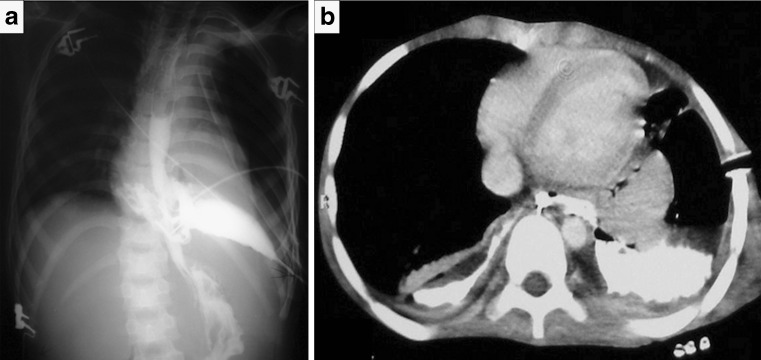
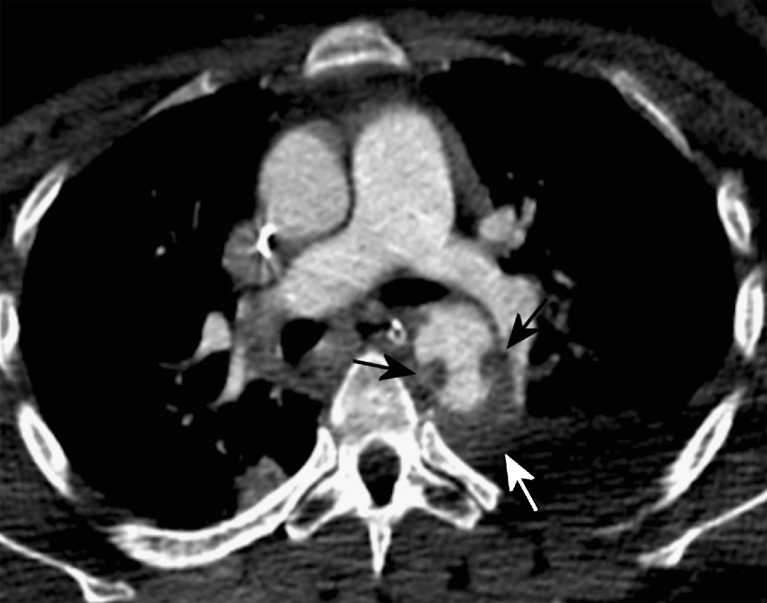
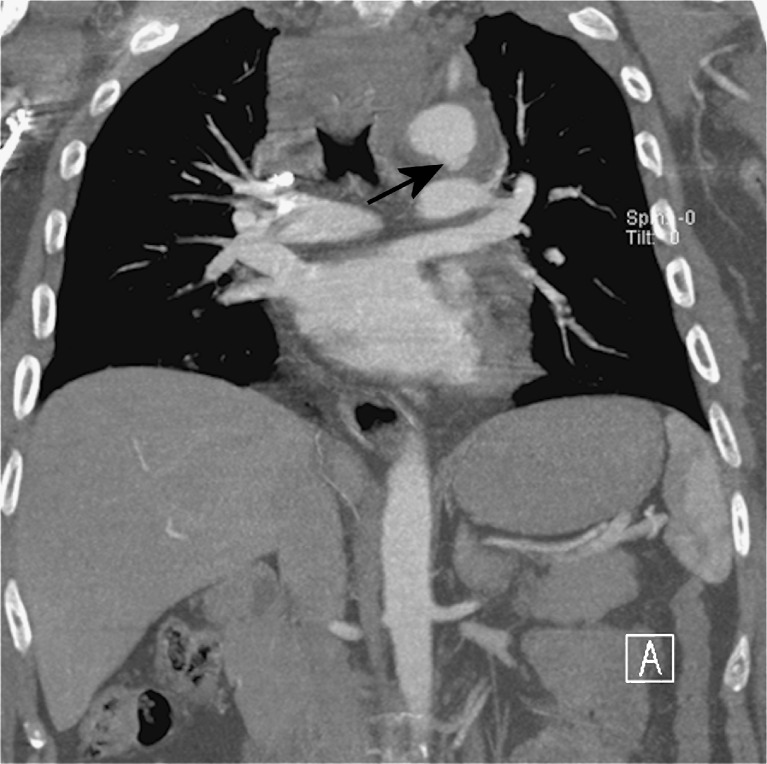
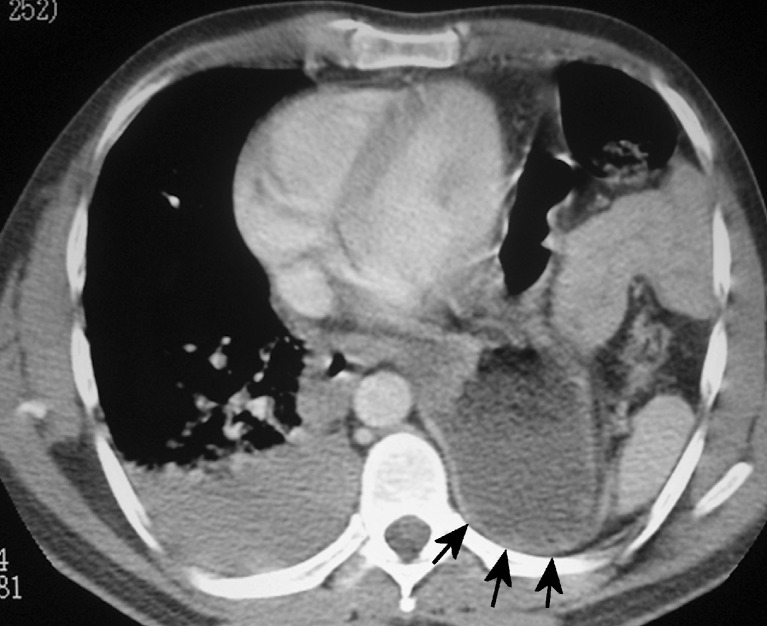
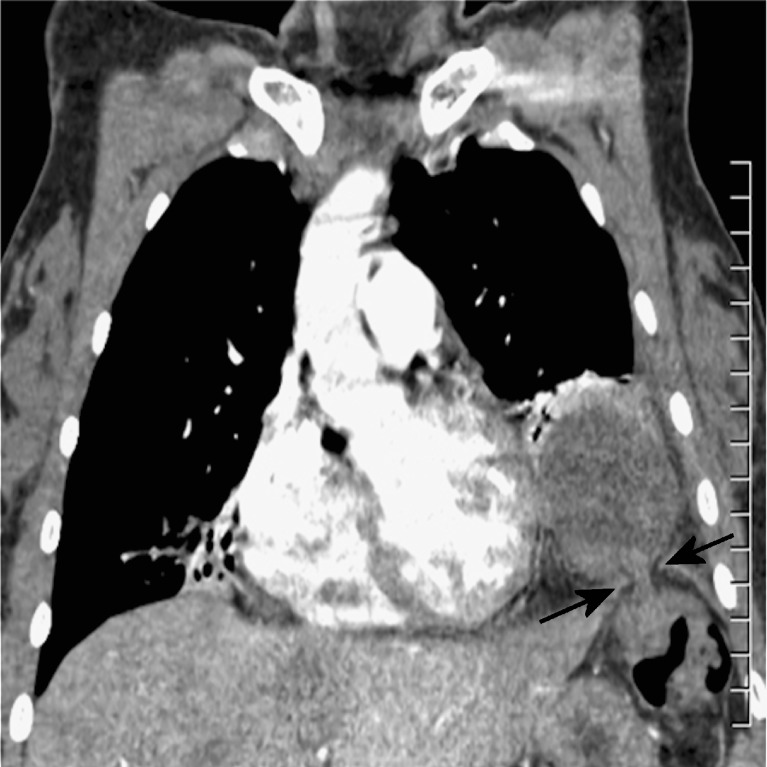
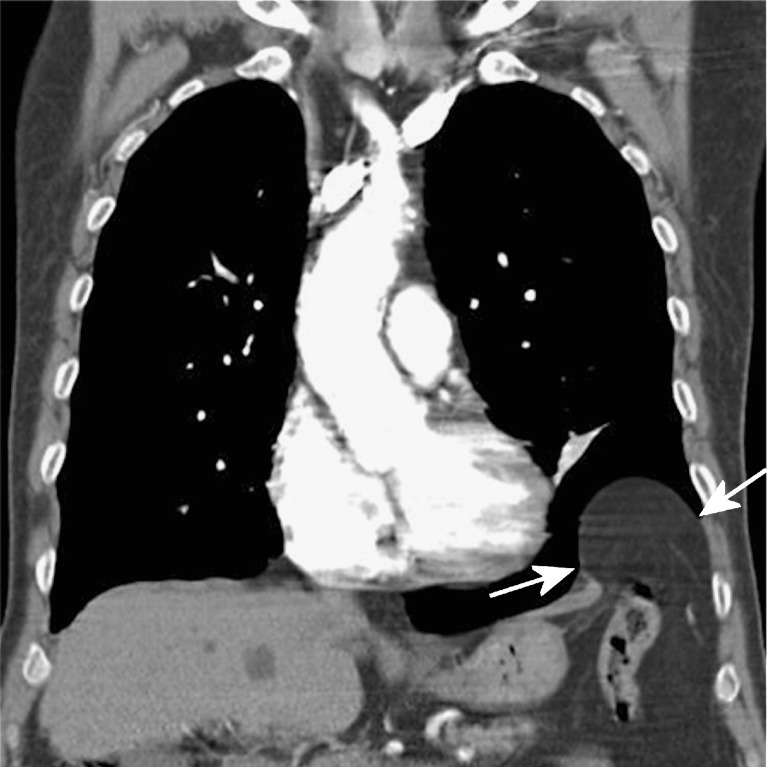
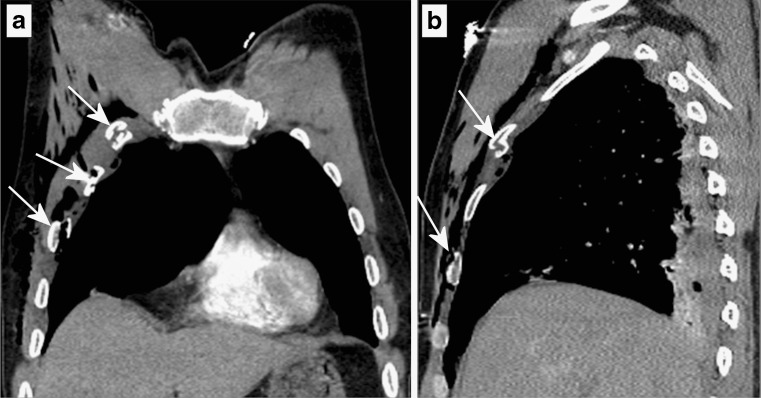
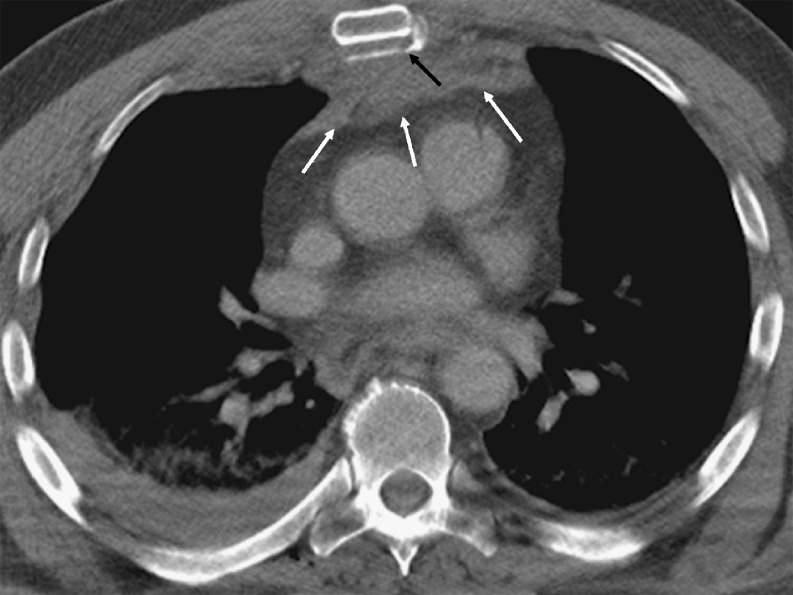
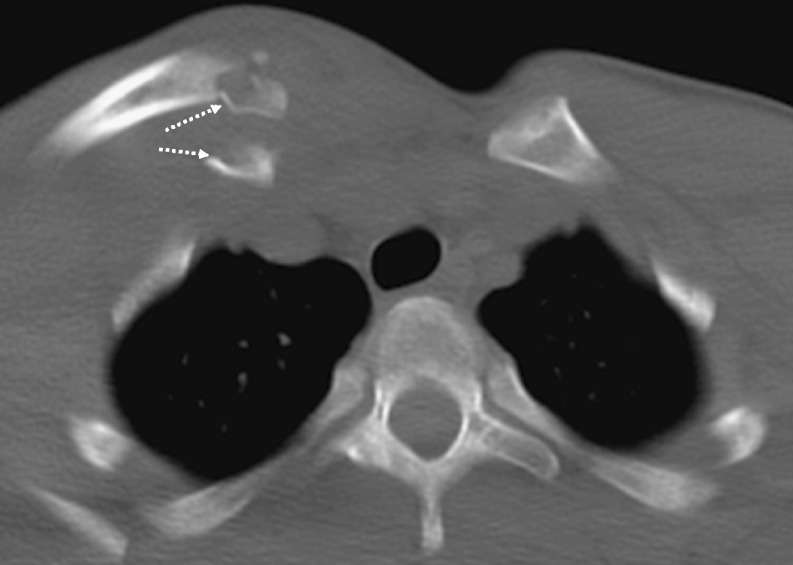
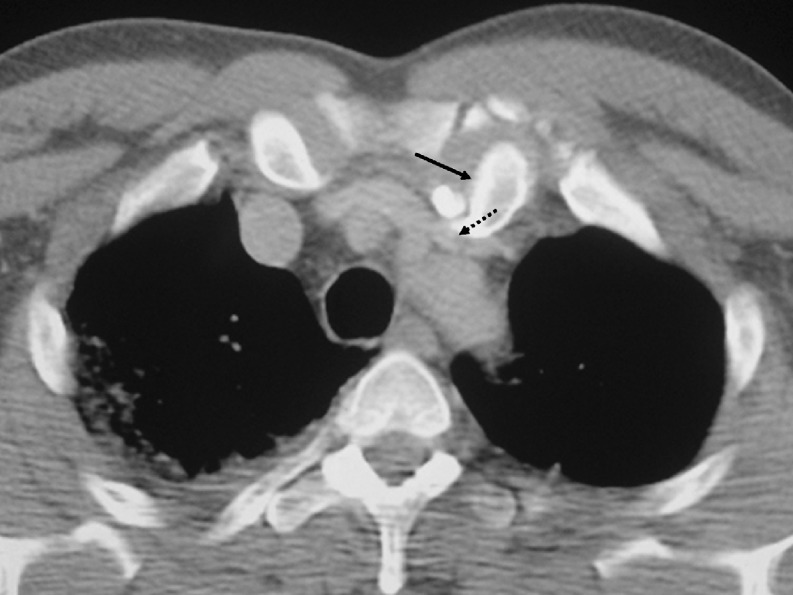
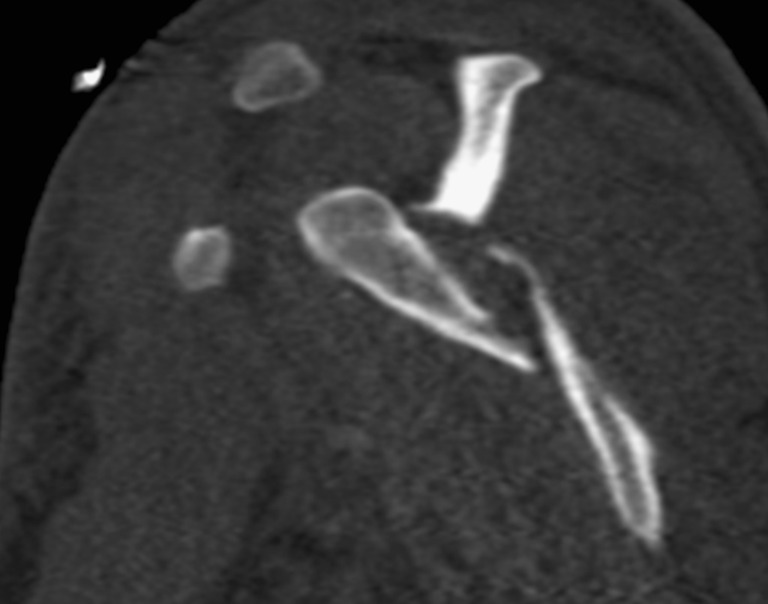
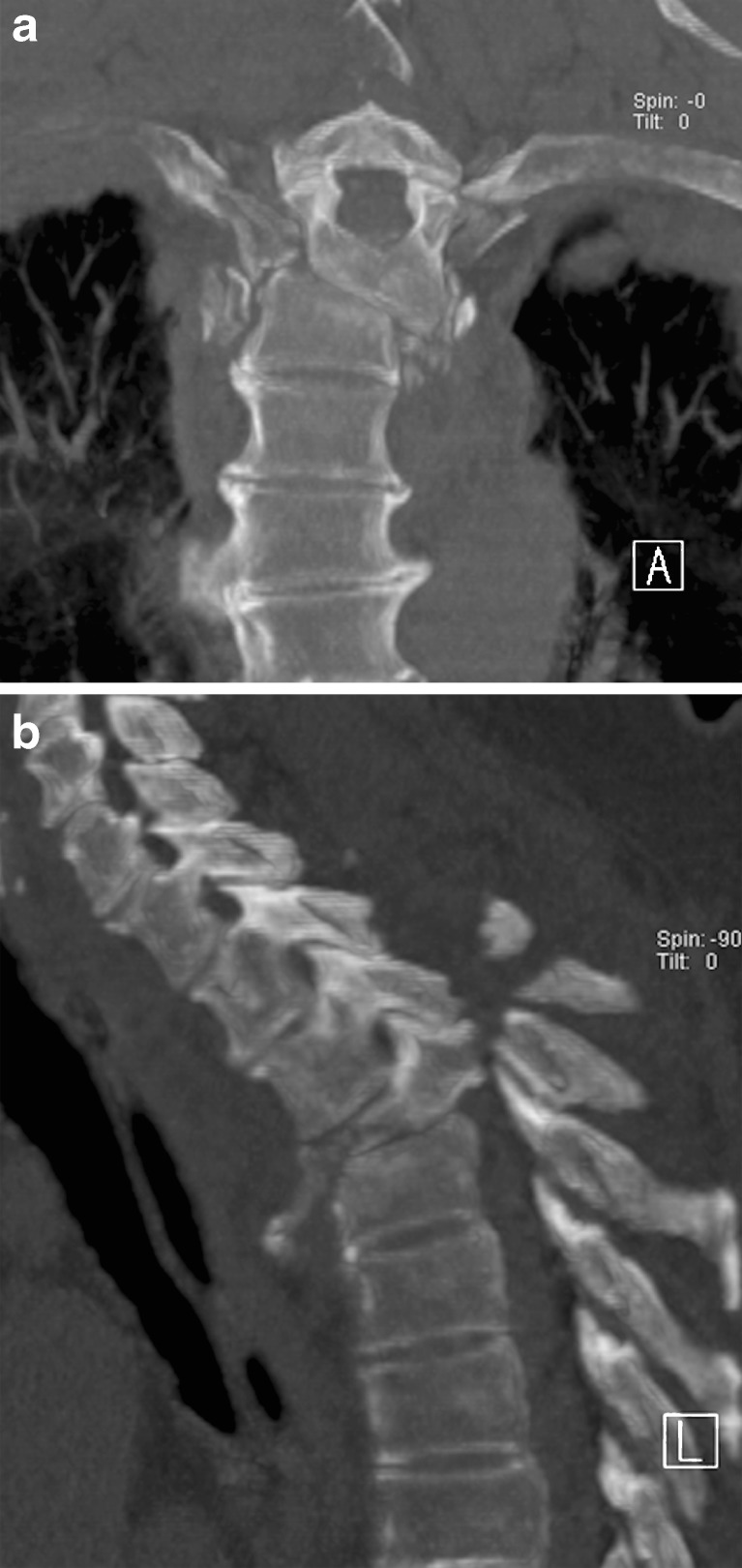
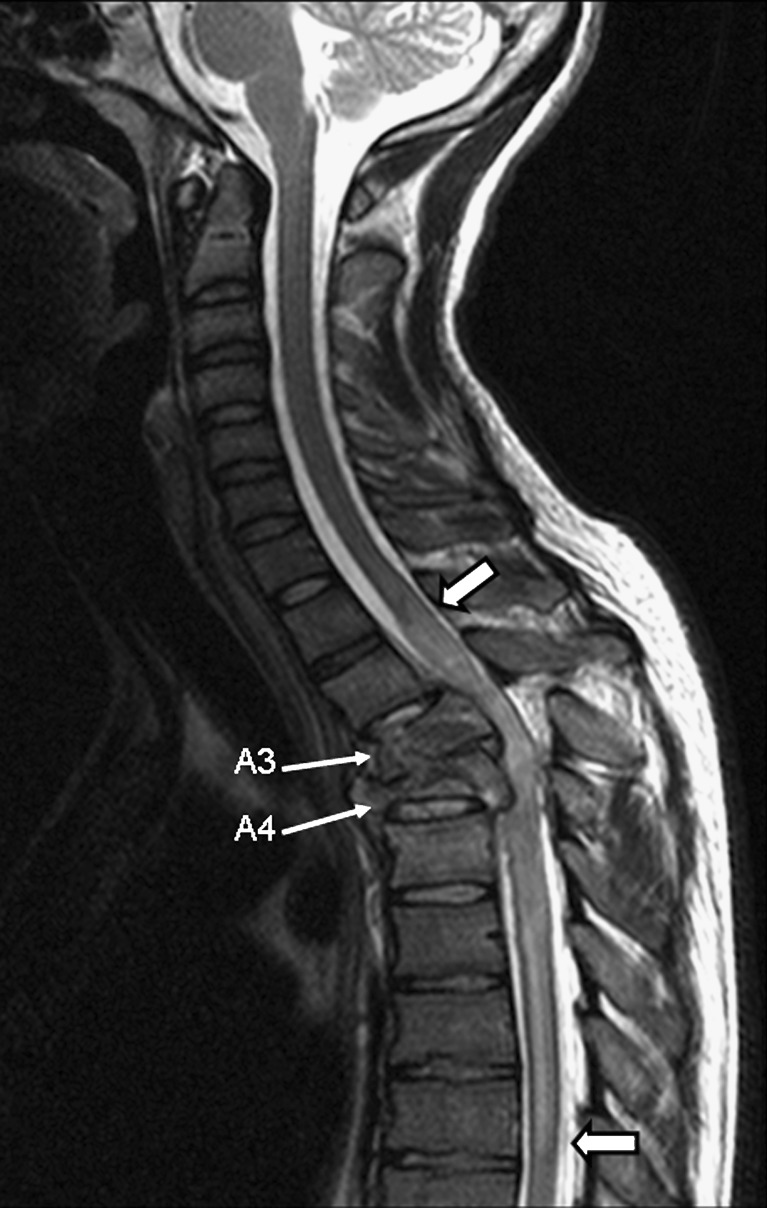
BACKGROUND: Thoracic injury overall is the third most common cause of trauma following injury to the head and extremities. Thoracic trauma has a high morbidity and mortality, accounting for approximately 25% of trauma-related deaths, second only to head trauma. More than 70% of cases of blunt thoracic trauma are due to motor vehicle collisions, with the remainder caused by falls or blows from blunt objects. METHODS: The mechanisms of injury, spectrum of abnormalities and radiological findings encountered in blunt thoracic trauma are categorised into injuries of the pleural space (pneumothorax, hemothorax), the lungs (pulmonary contusion, laceration and herniation), the airways (tracheobronchial lacerations, Macklin effect), the oesophagus, the heart, the aorta, the diaphragm and the chest wall (rib, scapular, sternal fractures and sternoclavicular dislocations). The possible coexistence of multiple types of injury in a single patient is stressed, and therefore systematic exclusion after thorough investigation of all types of injury is warranted. RESULTS: The superiority of CT over chest radiography in diagnosing chest trauma is well documented. Moreover, with the advent of MDCT the imaging time for trauma patients has been significantly reduced to several seconds, allowing more time for appropriate post-diagnosis care. CONCLUSION: High-quality multiplanar and volumetric reformatted CT images greatly improve the detection of injuries and enhance the understanding of mechanisms of trauma-related abnormalities.
Figures










References
-
- Clark DE, Fantus RJ, editors. National Trauma Data Bank (NTDB) Annual Report 2007. Chicago, IL: American College of Surgeons; 2007. pp. 1–64.
LinkOut - more resources
Full Text Sources
Other Literature Sources