

doi: 10.1007/s13244-011-0105-4.
Epub 2011 May 22.
Omental cakes: unusual aetiologies and CT appearances
- PMID: 22347961
- PMCID: PMC3259316
- DOI: 10.1007/s13244-011-0105-4
Item in Clipboard
Omental cakes: unusual aetiologies and CT appearances
Insights Imaging.
2011 Aug.
Abstract
BACKGROUND: Omental cakes typically are associated with ovarian carcinoma, as this is the most common malignant aetiology. Nonetheless, numerous other neoplasms, as well as infectious and benign processes, can produce omental cakes. METHODS: A broader knowledge of the various causes of omental cakes is valuable diagnostically and to direct appropriate clinical management. RESULTS: We present a spectrum of both common and unusual aetiologies that demonstrate the variable computed tomographic appearances of omental cakes. CONCLUSION: The anatomy and embryology are discussed, as well as the importance of biopsy when the aetiology of omental cakes is uncertain.
Figures
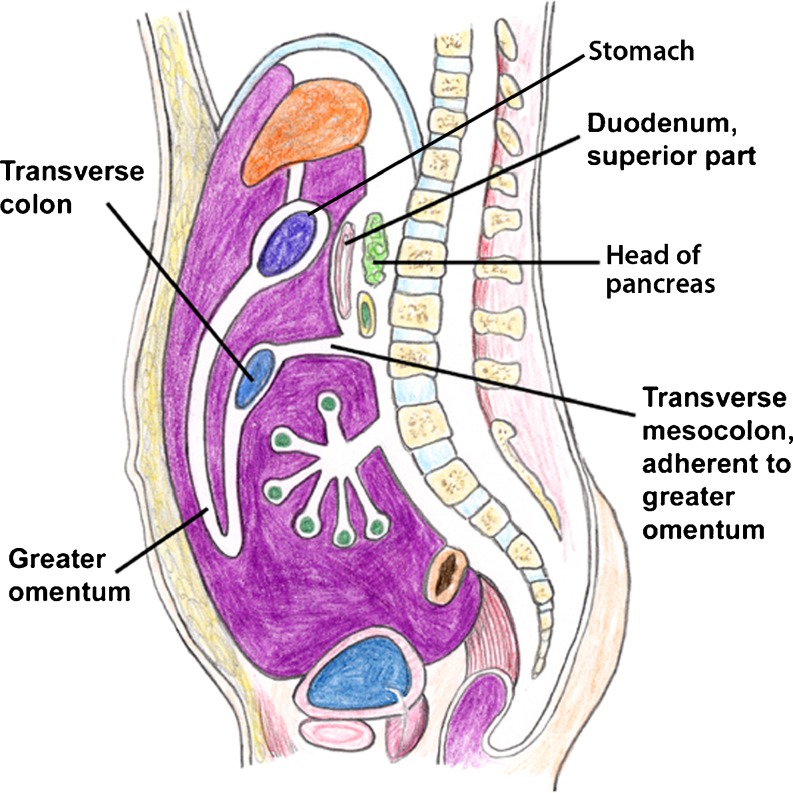
Schematic sagittal diagram demonstrating the anatomy of the greater omentum (Modified and reprinted with permission from [2])
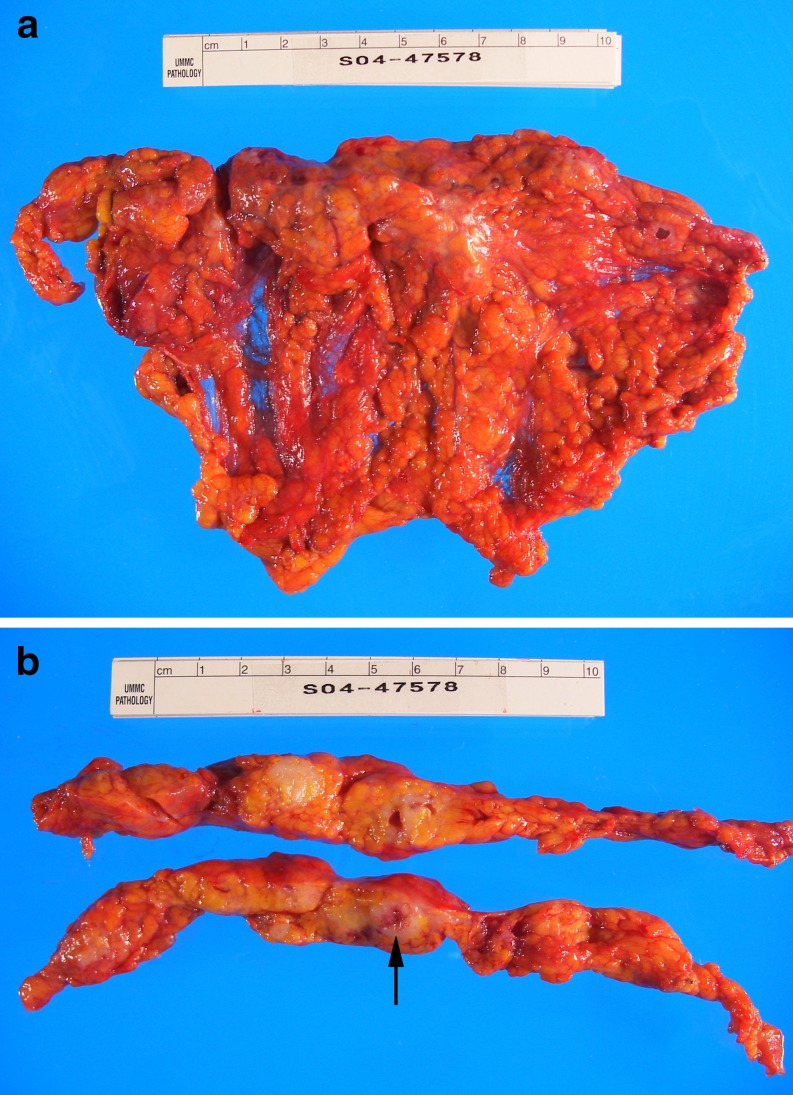
(a,b). Adenocarcinoma of the vulva in a 55-year-old woman. a Gross omental cake specimen with an 8-cm irregular firm nodular lesion at the superior border. b Transverse sections of the omentum show that the lesion is solid, tan-white with scattered foci of hemorrhage (arrow)
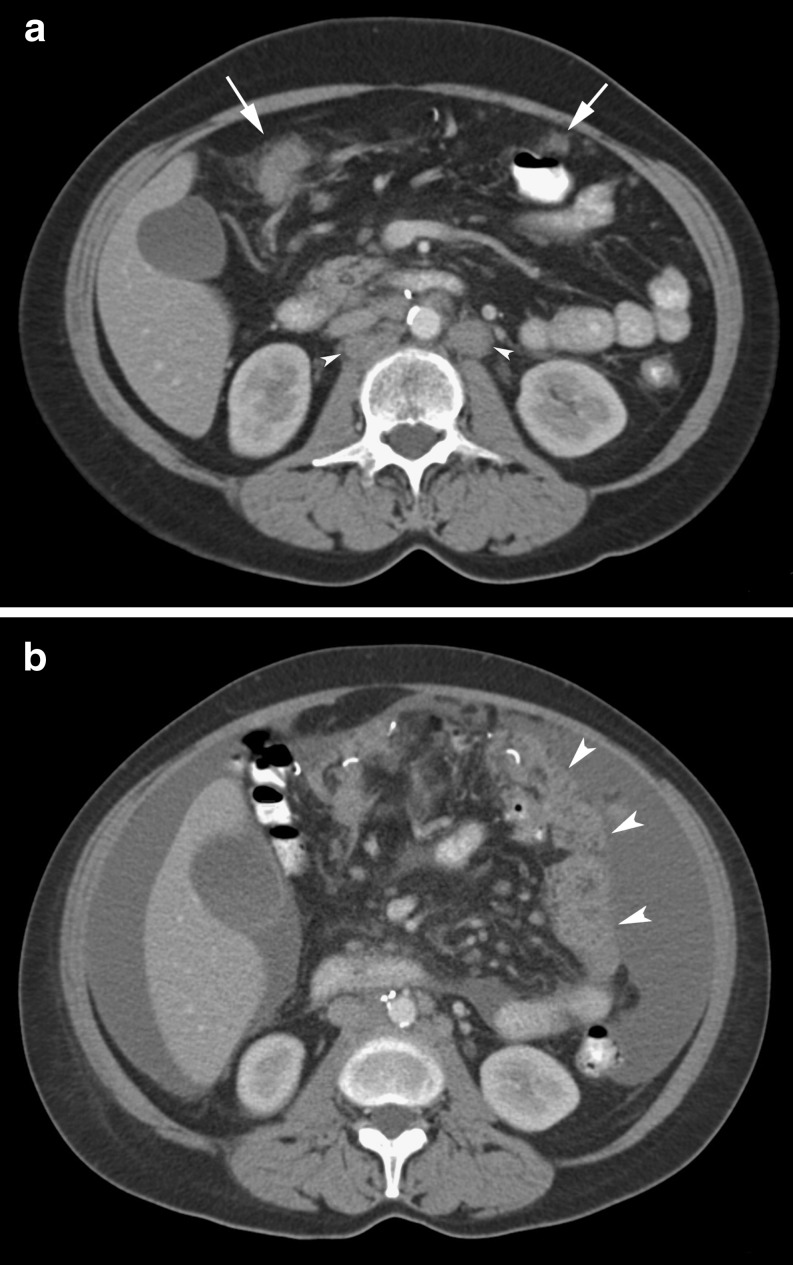
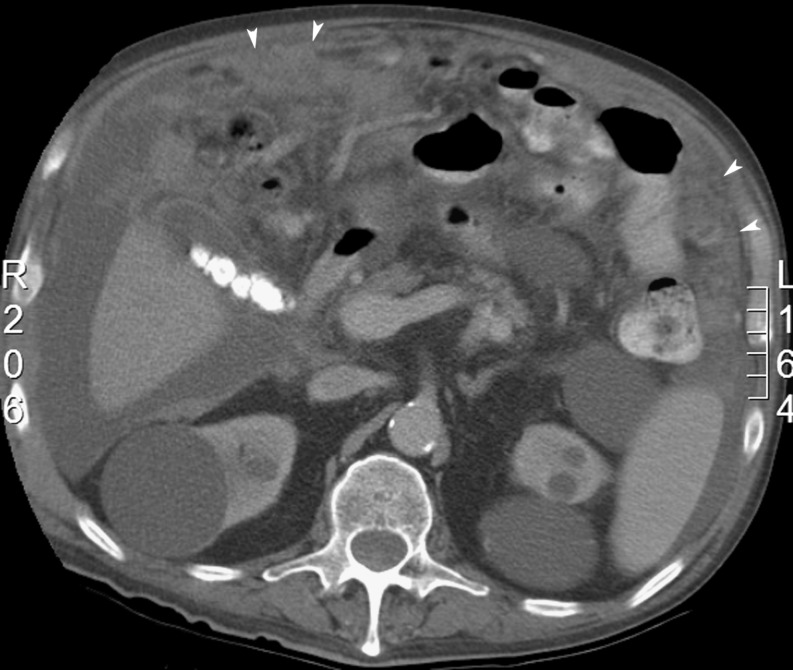
(a,b). Ovarian cancer in a 47-year-old woman demonstrating progresssion of omental cake. a Initial CT image shows early infiltration and nodularity of the omentum (arrows) and retroperitoneal adenopathy (arrowheads). b Interval progression of disease with ascites and the mass-like omental cake (arrowheads) in the remaining omentum after a partial omentectomy on a CT scan 3 months later
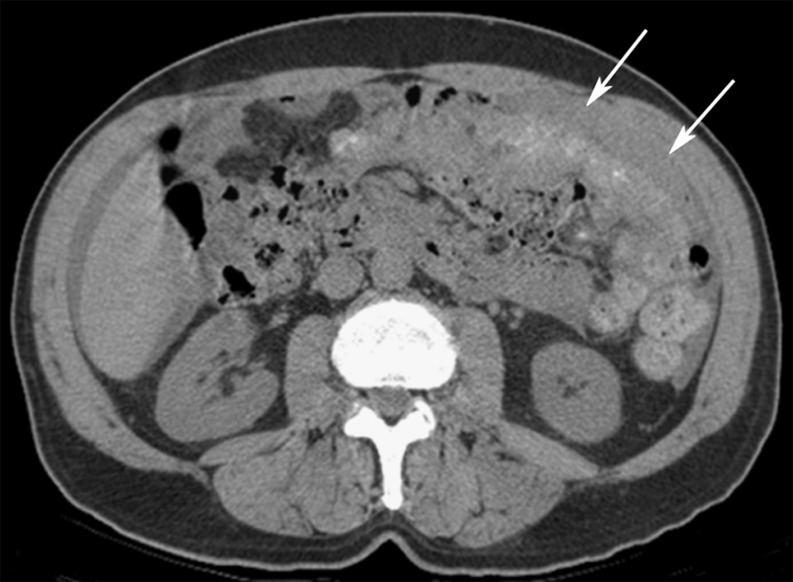
Ovarian cancer in a 51-year-old woman. CT image shows extensive omental thickening (arrows) and ascites
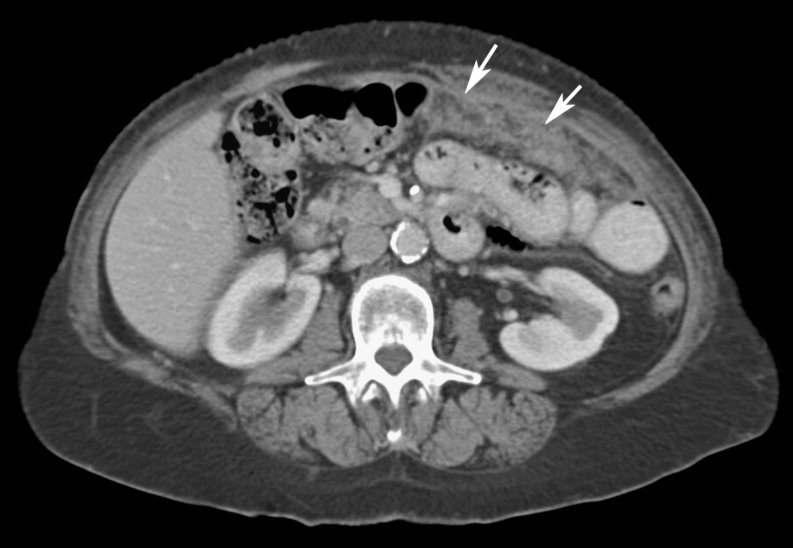
Colon cancer in a 65-year-old man. CT image demonstrates a thick omental cake in the left anterior abdomen (arrows). Peripheral ascites is also present, predominantly on the right side
Pancreatic adenocarcinoma in a 58-year-old man. CT image shows multiple, ill-defined, soft tissue nodules and masses (arrows) permeating the omental fat. Ascites is also present in the right paracolic gutter

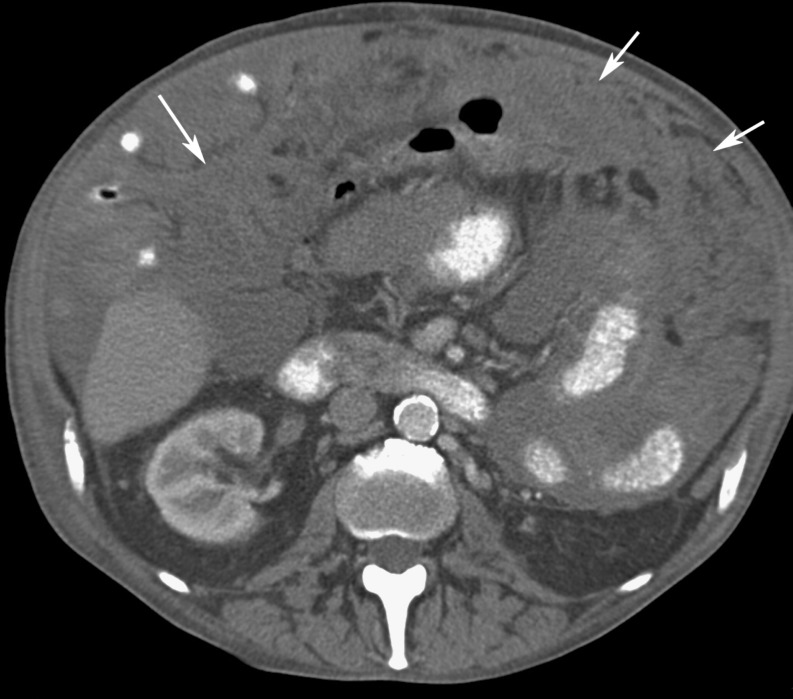
Gastric cancer in a 53-year-old woman. CT image demonstrates diffuse linear infiltration, nodularity, and thickening of the omentum (arrows)

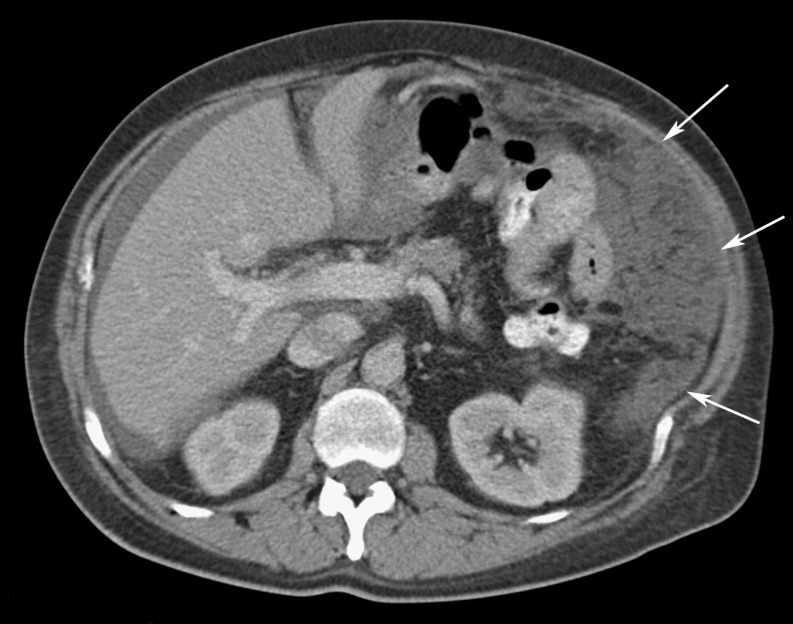
Renal cell carcinoma in a 62-year-old man. CT image shows extensive soft tissue nodules present within the omentum (arrows) and the retroperitoneum. A right nephrectomy with surgical clips is seen in the right renal fossa, and ascites is also seen on the right

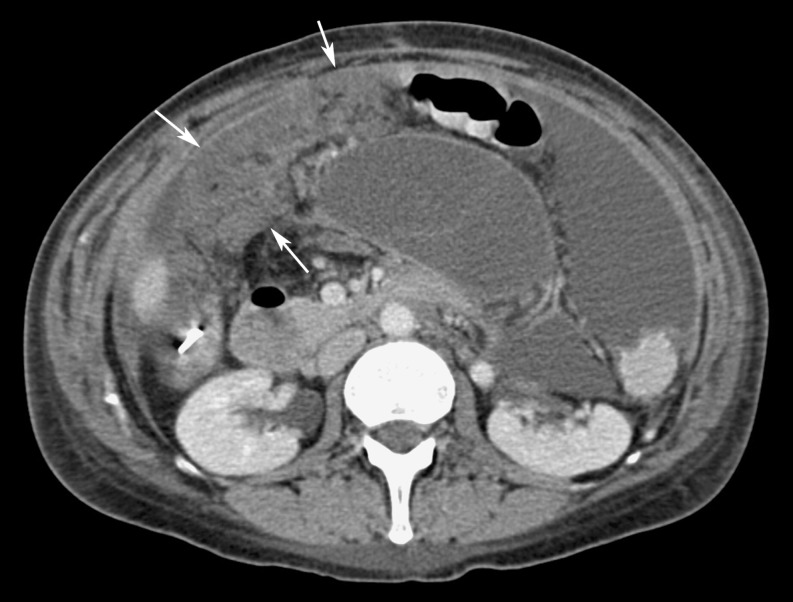
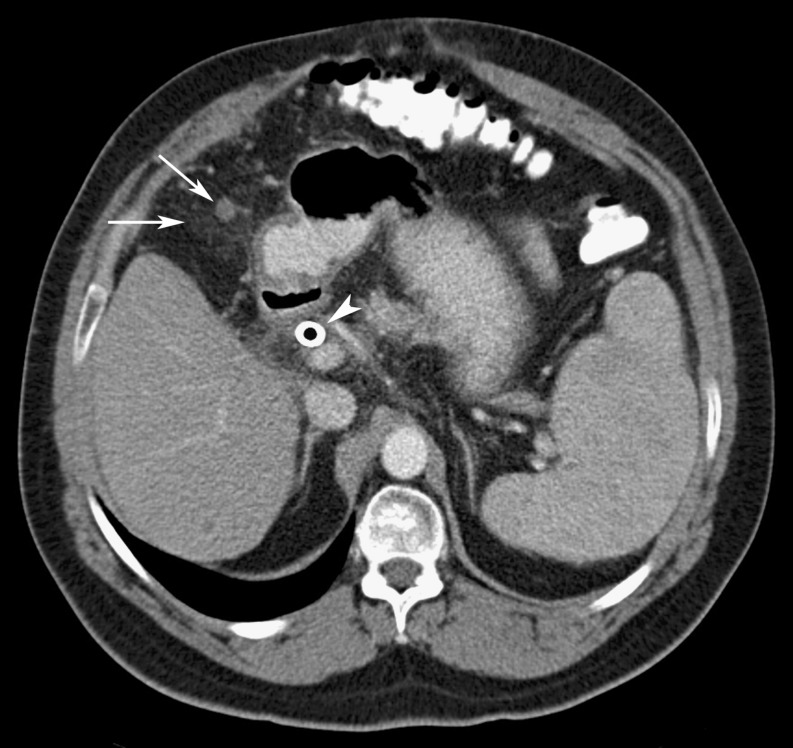
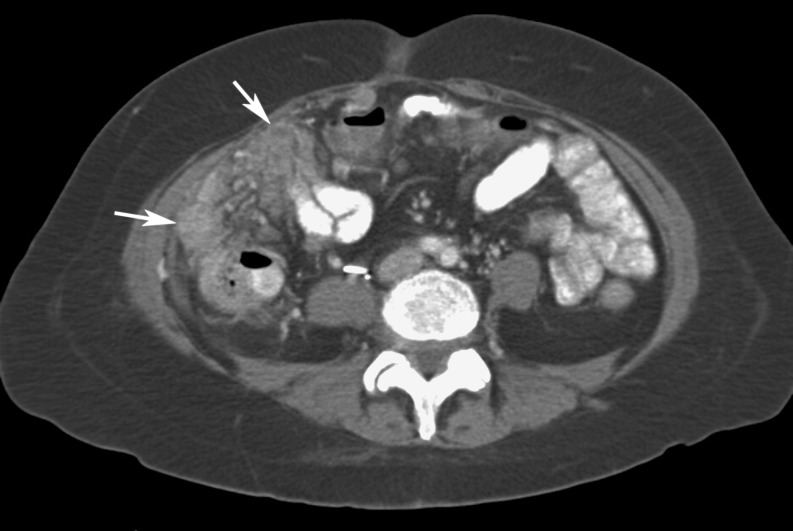
Gallbladder carcinoma in a 70-year-old woman. CT image illustrates an omental cake anterior to the liver with infiltration and nodularity of the omental fat (arrows). The tumour also infiltrates the fat of the lesser sac (arrowheads)
Cholangiocarcinoma in a 56-year-old man. CT image shows omental involvement with infiltration and nodules (arrows). A biliary stent is also present (arrowhead). Splenomegaly is present
Fallopian tube carcinoma in a 45-year-old woman. CT image demonstrates omental involvement (arrows) as infiltration of the fat, nodularity, and coalescence of the nodules form an omental cake

Endometrial adenocarcinoma in a 50-year-old woman. CT image shows multiple nodular metastases present within the omentum (arrows) and along the peritoneal surface, the result of intraperitoneal seeding. Hepatomegaly and retroperitoneal metastases are present

Prostate cancer in a 75-year-old man. CT image demonstrates omental infiltration (arrows) seen in the absence of ascites or other signs of peritoneal carcinomatosis. Note is made of an inferior vena cava filter

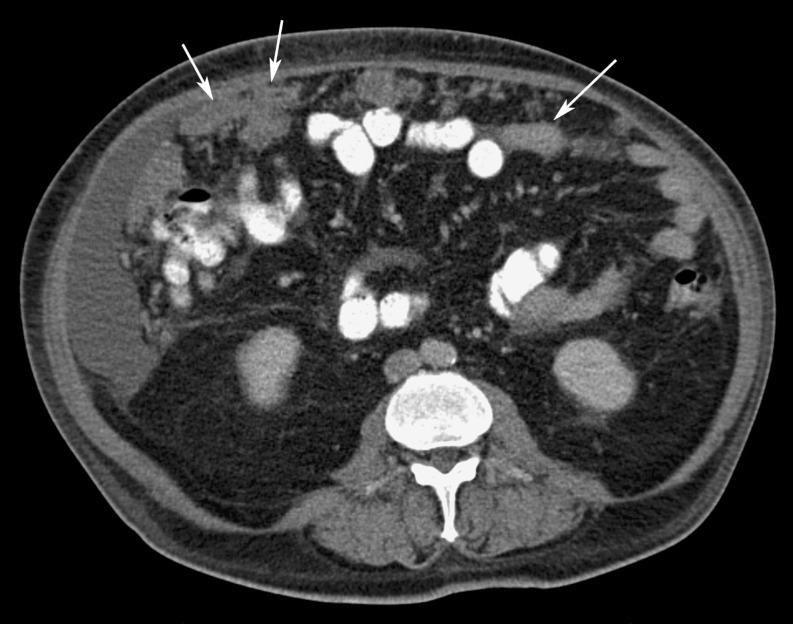
Urothelial carcinoma of the bladder in a 59-year-old man. CT image shows extensive diffuse omental involvement (arrows), including the surfaces of the adjacent bowel

Breast cancer in a 45-year-old woman. CT image illustrates peritoneal carcinomatosis with ascites, peritoneal thickening, nodularity (curved arrow), and omental cake (arrowheads). Note also the shrunken liver (arrows) with pseudocirrhosis appearance seen after treatment for liver metastases from breast cancer

Non-small cell lung cancer in a 65-year-old man. CT image demonstrates hematogenous metastases seeding the omentum as seen in this omental cake (arrows) adjacent to the spleen and left upper quadrant. There are small bilateral pleural effusions
Non-Hodgkin’s lymphoma in a 70-year-old man. CT image shows omental cakes (arrowheads) manifested as ill-defined areas of soft tissue anteriorly and peripherally in the abdomen. Multiple renal cysts and calcified gallstones are present, as is ascites
Primary mesothelioma in a 52-year-old man. CT image shows a thin omental cake (arrows) in the anterior abdomen with a small amount of ascites in the left paracolic gutter and perihepatic spaces
Testicular mesothelioma in a 53-year-old man. CT image shows an omental cake (arrows) in the anterior abdomen
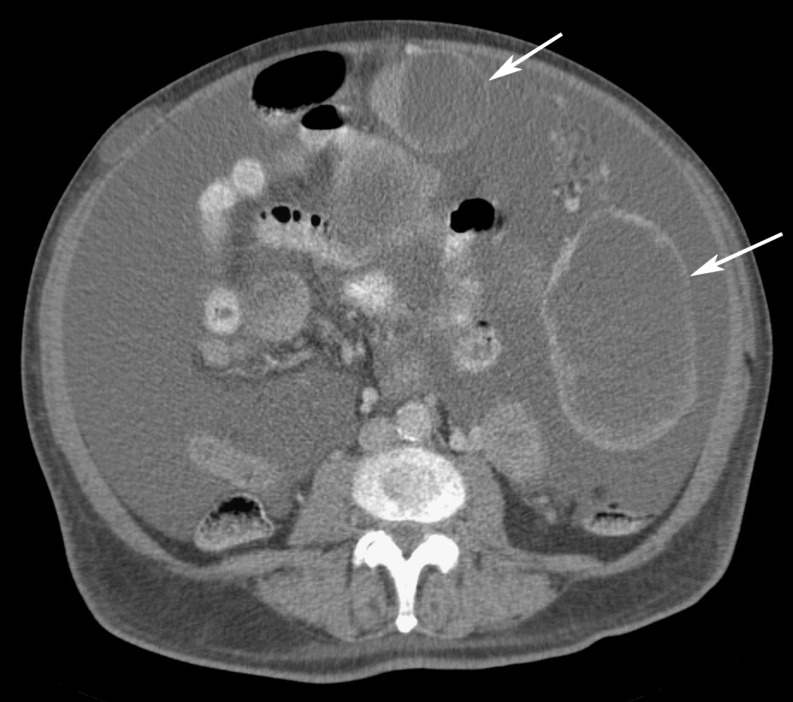
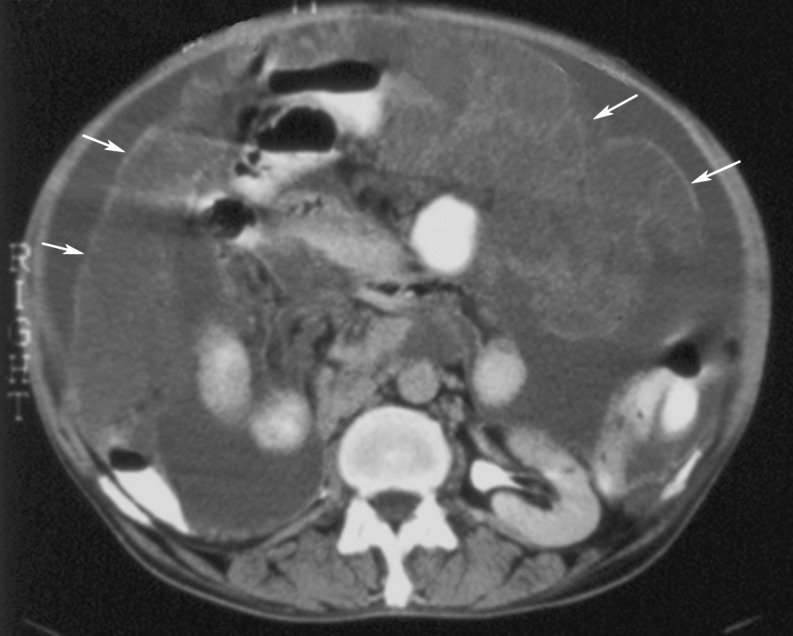
Gastrointestinal stromal tumour (GIST) in a 45-year-old man. CT image shows large, cystic-appearing masses (arrows), some involving the omentum, and a large volume of ascites. The patient had been treated with imatinib mesylate (Gleevec; Novartis, New York, NY) that led to the cystic changes. There is a subcutaneous implant in the right anterior abdominal wall
Liposarcoma in a 56-year-old man. CT image demonstrates multiple, clustered, nodular metastases present within the omentum seen in the right abdomen (arrows)
Tuberculosis in a 51-year-old man. CT image demonstrates ascites and large, low-attenuation omental macronodules covered with a thin omental line (arrows)
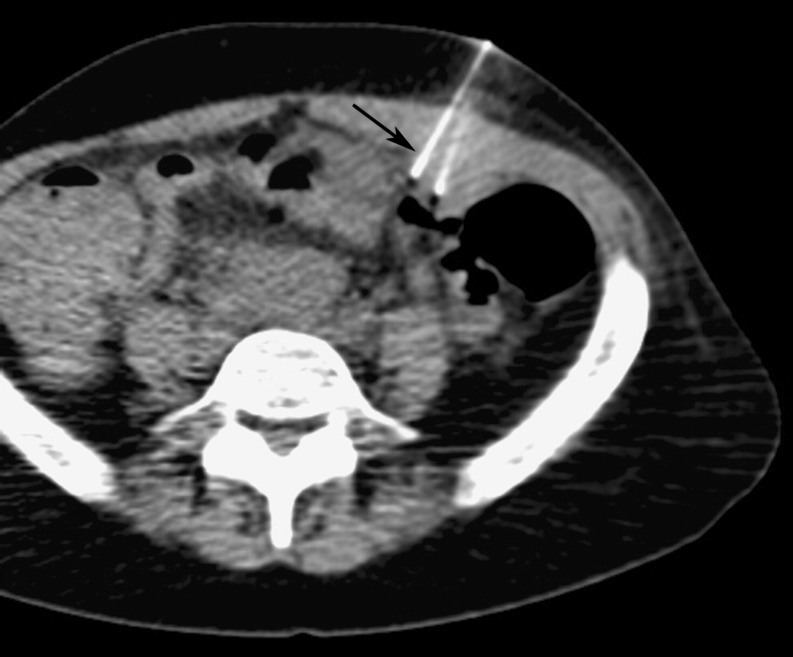
41-year-old woman with AIDS, an ovarian mass, and omental cake: CT fluoroscopic-guided percutaneous biopsy of the omental thickening using a 22-g needle revealed Actinomyces israelii, but no evidence of malignancy
Coccidioidomycosis in a 43-year-old woman. CT image shows an omental nodule in the right anterior abdomen (arrow) and mesenteric lymph nodes (arrowheads). (Courtesy of Dr. Arash Heidari)
Myelofibrosis in a 66-year-old man with a history of splenectomy. CT image shows extensive omental infiltration (arrows) with areas of nodularity and ascites. Oral contrast is noted in bowel loops. Biopsy revealed extramedullary hematopoiesis. Benign omental cakes are indistinguishable from those caused by malignancy

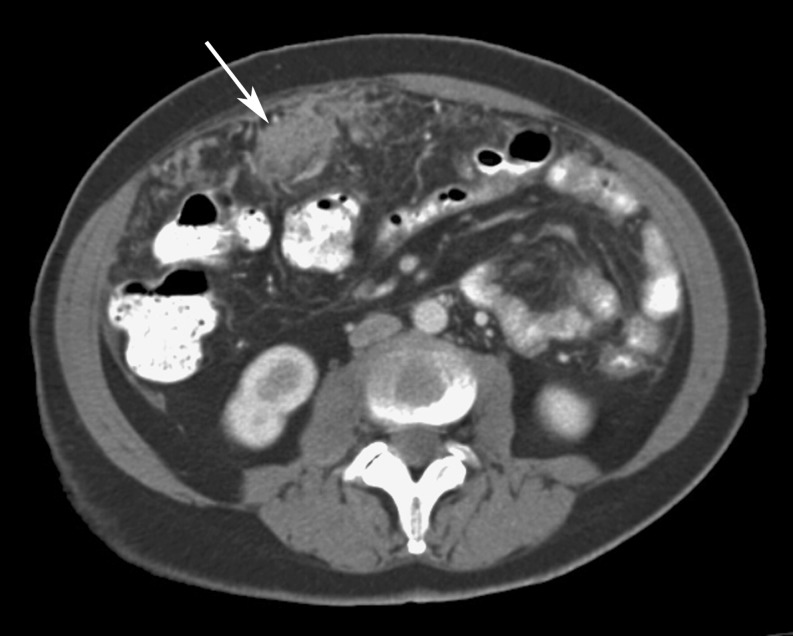
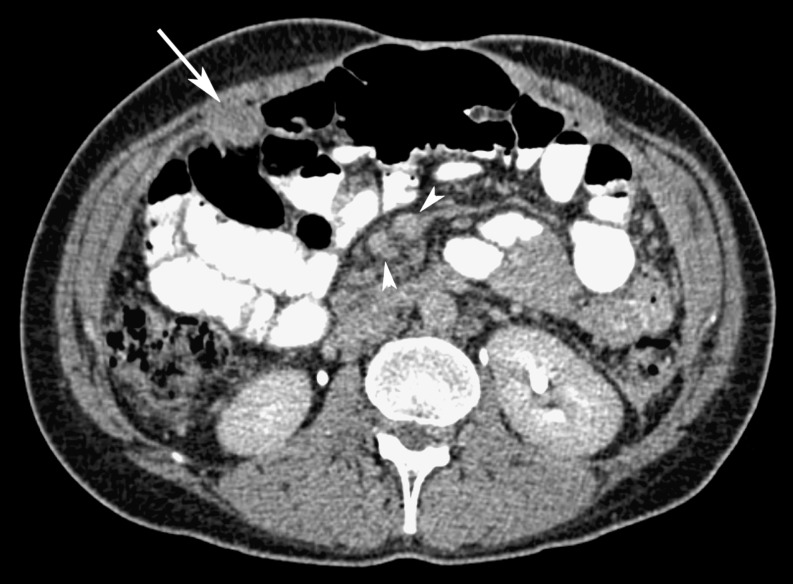
Unknown primary cancer and omental cake in a 65-year-old man. CT fluoroscopic-guided biopsy of the omental cake using a 22-g needle (arrow) revealed adenocarcinoma, with the primary being in the colon
Similar articles
-
Omental cakes in American Burkitt lymphoma. Computed tomography demonstration.Clin Imaging. 1989 Jun;13(2):117-8. doi: 10.1016/0899-7071(89)90090-9. Clin Imaging. 1989. PMID: 2766073
-
Postoperative omental infarction following colonic resection.Clin Radiol. 2012 Feb;67(2):134-9. doi: 10.1016/j.crad.2011.07.051. Epub 2011 Sep 13. Clin Radiol. 2012. PMID: 21917243
-
Gastric involvement by omental cakes: radiographic findings.Gastrointest Radiol. 1986;11(3):223-8. doi: 10.1007/BF02035078. Gastrointest Radiol. 1986. PMID: 3743942
-
Predictive value of omental thickness on ultrasonography for diagnosis of unexplained ascites, an Egyptian centre study.Asian J Surg. 2020 Jan;43(1):13-19. doi: 10.1016/j.asjsur.2019.03.004. Epub 2019 Mar 22. Asian J Surg. 2020. PMID: 30910377 Review.
-
Extragonadal omental teratoma: a case report.J Obstet Gynaecol Res. 2014 Feb;40(2):618-21. doi: 10.1111/jog.12198. Epub 2013 Oct 22. J Obstet Gynaecol Res. 2014. PMID: 24147579 Review.
Cited by
-
Imaging patterns of wall thickening type of gallbladder cancer.Clin Exp Hepatol. 2022 Dec;8(4):255-266. doi: 10.5114/ceh.2022.122285. Epub 2022 Dec 28. Clin Exp Hepatol. 2022. PMID: 36683868 Free PMC article. Review.
-
Peritoneal tuberculosis mimicking carcinomatous ascites in a child living in a low prevalence country: a case report.Ital J Pediatr. 2020 Apr 19;46(1):49. doi: 10.1186/s13052-020-0816-6. Ital J Pediatr. 2020. PMID: 32307013 Free PMC article.
-
A case of Waldenström's macroglobulinemia treated using clarithromycin and prednisolone.Transl Clin Pharmacol. 2017 Sep;25(3):134-137. doi: 10.12793/tcp.2017.25.3.134. Epub 2017 Sep 15. Transl Clin Pharmacol. 2017. PMID: 32095463 Free PMC article.
-
Diagnostic Accuracy of Different Computed Tomography Signs for Differentiating Between Malignant and Cirrhotic Ascites Keeping Ascitic Fluid Cytology as Gold Standard.Cureus. 2021 Dec 7;13(12):e20254. doi: 10.7759/cureus.20254. eCollection 2021 Dec. Cureus. 2021. PMID: 35004063 Free PMC article.
-
Negative Serum Ascites Albumin Gradient (SAAG) in the Setting of Cholangiocarcinoma: A Case Report.Cureus. 2023 Apr 13;15(4):e37528. doi: 10.7759/cureus.37528. eCollection 2023 Apr. Cureus. 2023. PMID: 37193465 Free PMC article.
References
-
- Miller Q, Kline AL (2008) Solid Omental Tumours. eMedicine.com http://emedicine.medscape.com/article/193622-overview. Image modified and reprinted with permission from eMedicine.com, 2010
-
- Sompayrac SW, Mindelzun RE, Silverman PM, Sze R. The greater omentum. AJR Am J Roentgenol. 1997;168:683–687. - PubMed
-
- Krist LFG, Kerremans M, Broekhuis-Fluitsma DM, Eestermans IL, Meyer S, Beelen RHJ. Milky spots in the greater omentum are predominant sites of local tumour cell proliferation and accumulation in the peritoneal cavity. Cancer Immunol Immunother. 1998;47:205–212. doi: 10.1007/s002620050522. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources