

doi: 10.1007/s13244-011-0087-2.
Epub 2011 May 1.
Pseudotumoural soft tissue lesions of the foot and ankle: a pictorial review
- PMID: 22347966
- PMCID: PMC3259410
- DOI: 10.1007/s13244-011-0087-2
Item in Clipboard
Pseudotumoural soft tissue lesions of the foot and ankle: a pictorial review
Insights Imaging.
2011 Aug.
Abstract
In the foot and ankle region, benign neoplasms and pseudotumoural soft tissue lesions are significantly more frequent than malignant tumours. The pseudotumoural lesions constitute a heterogeneous group, with highly varied aetiology and histopathology. This article reviews the imaging features of the most common pseudotumours of the soft tissues in the foot and ankle. Although the imaging characteristics of several of the lesions discussed are non-specific, combining them with lesion location and clinical features allows the radiologist to suggest a specific diagnosis in most cases.
Figures
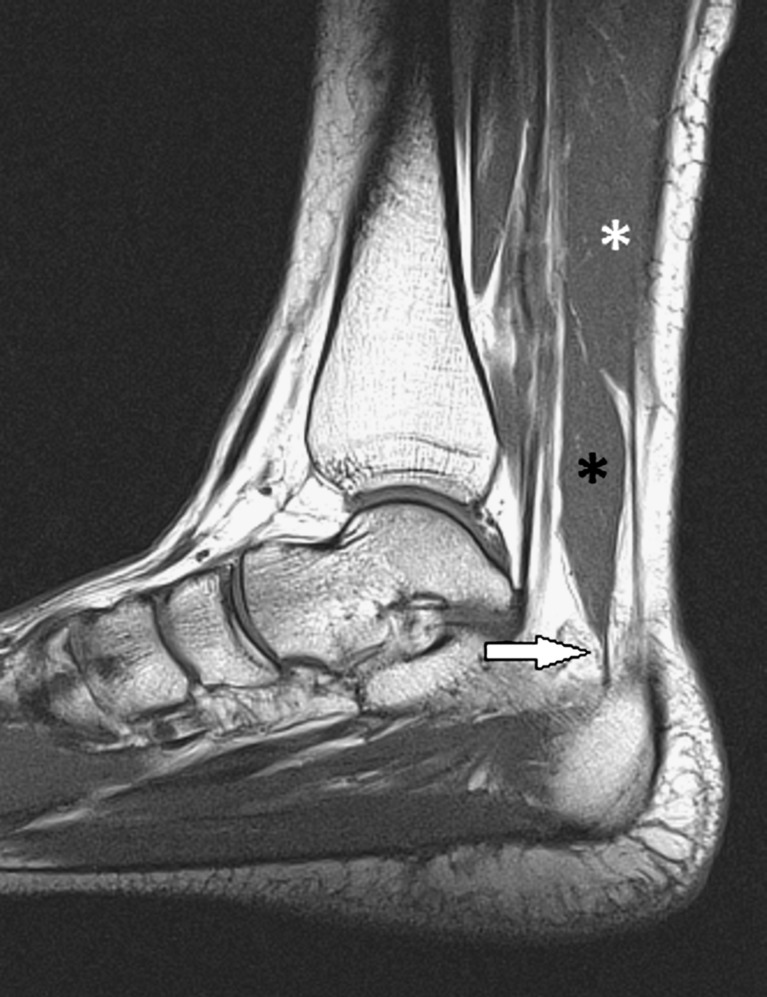
Accessory muscle. Sagittal T1-WI. An accessory soleus (black asterisk) is seen anterior-inferior to the soleus muscle (white asterisk), arising from the tibia (origin not shown) and with a tendinous insertion onto the superior surface of the calcaneus anteromedial to the Achilles tendon (arrow). This is just one of the five types of accessory soleus that have been described on the basis of insertion characteristics
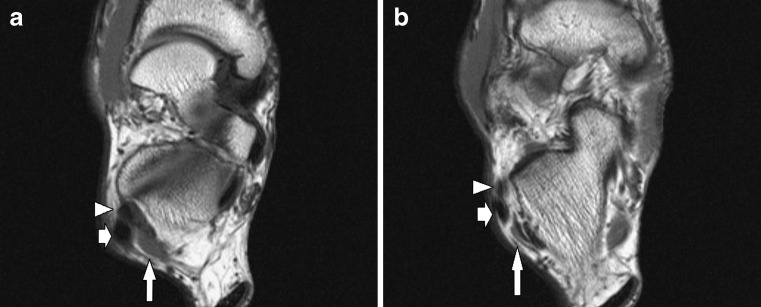
Accessory muscle: peroneus quartus. Axial T1-WI at the level of the subtalar joint (a) and slightly below (b). Peroneus quartus (long arrow) positioned posteromedial to tendons of the long (short arrow) and short (arrowhead) peroneal muscle. Several types of peroneus quartus are described based on the distal insertion, which can be onto the peroneal tubercle or the retrotrochlear eminence of the calcaneus, and less frequently the cuboid, the peroneus longus or the inferior peroneal retinaculum
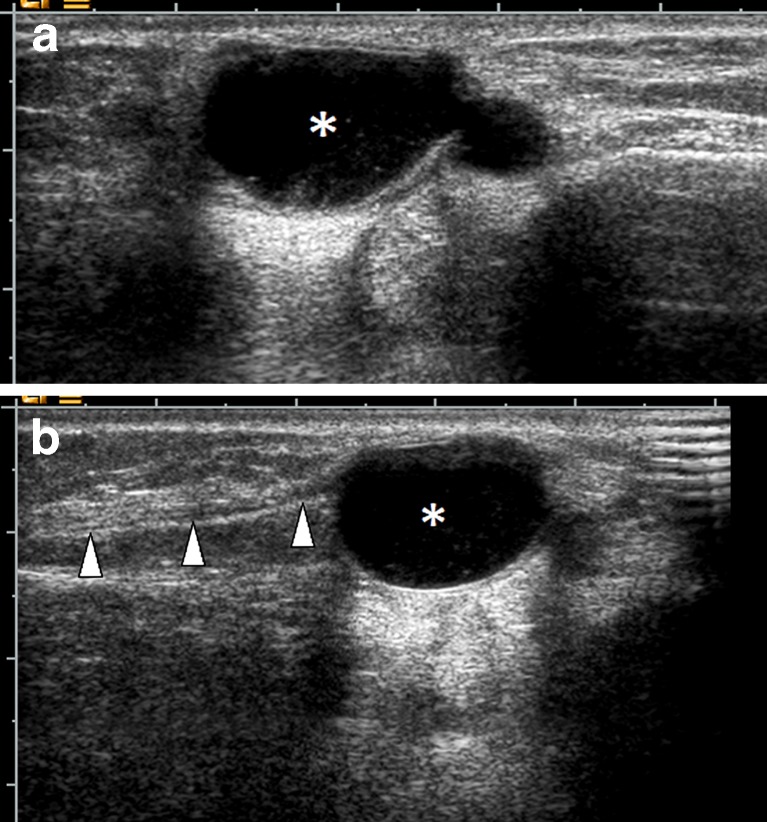
Synovial cyst. A 34-year-old female patient with lateral foot pain and soft tissue mass posterior to the lateral malleolus. Ultrasound examination in the paracoronal (a) and coronal plane (b) demonstrates a well-circumscribed, bilobular, mostly anechogenic lesion (asterisk) with posterior acoustic enhancement, correlating with a cystic nature. Some echogenic debris is present in the dependent part of the lesion. The lesion causes displacement of the sural nerve (arrowheads), causing lateral foot pain
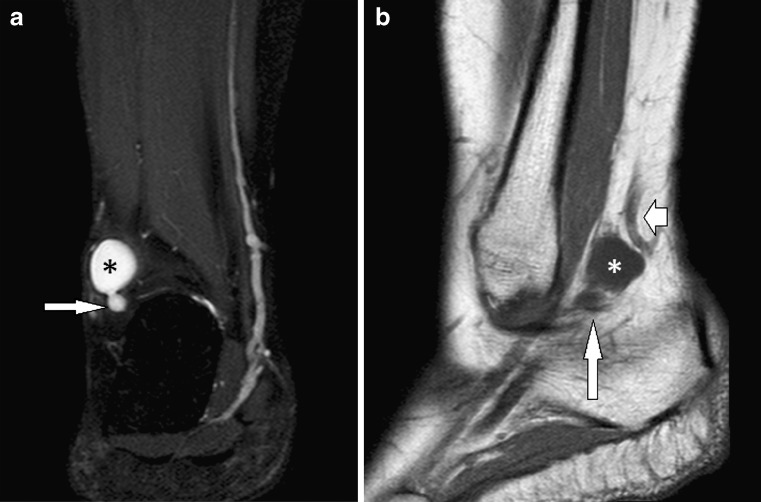
Synovial cyst. Same patient as in Fig. 3. Coronal fat-suppressed T2-WI (a) and sagittal T1-WI (b): well-circumscribed, bilobar lesion (asterisk) with high signal intensity (SI) on T2-WI and low SI on T1-WI. The smaller “lobe” (long arrow) extends caudally towards the posterior facet of the subtalar joint. The cyst causes displacement of the small saphenous vein (short arrow)
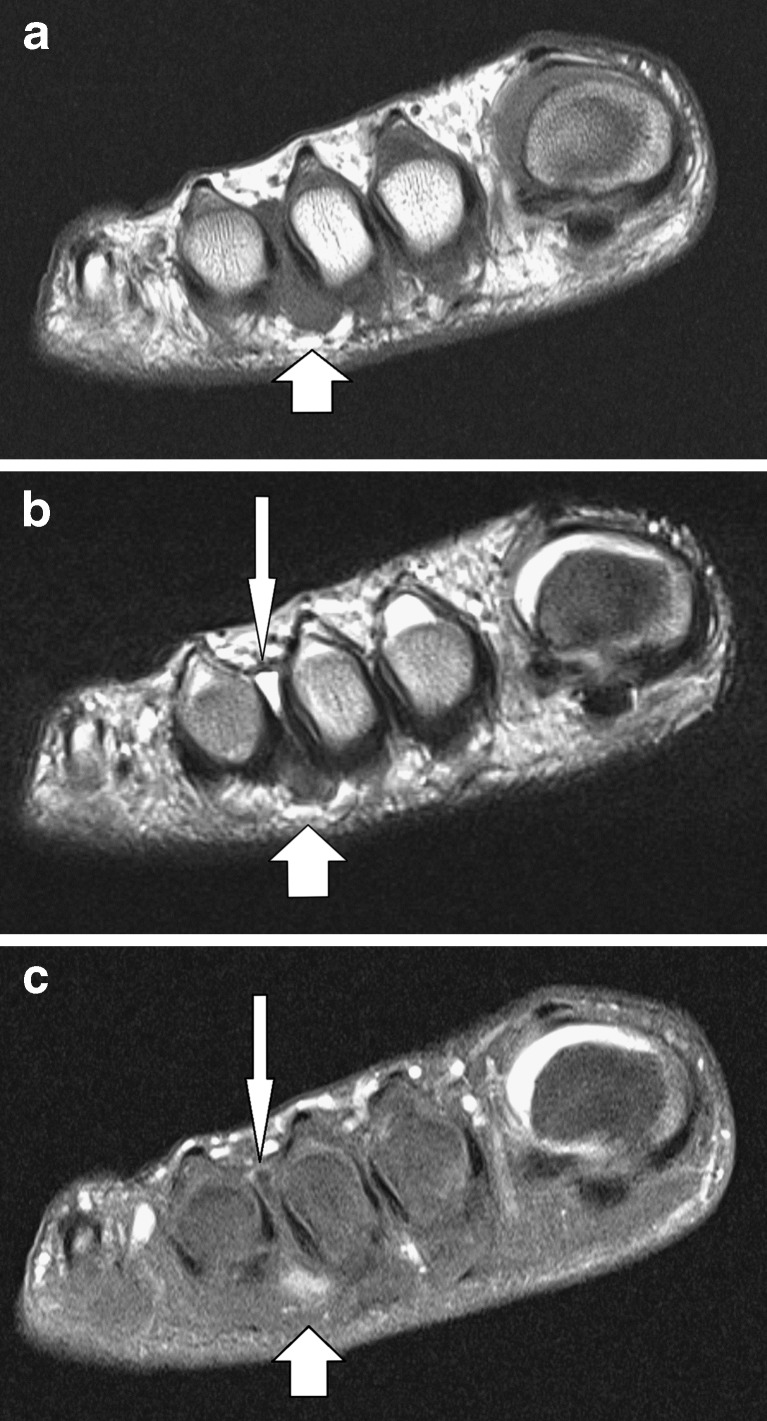
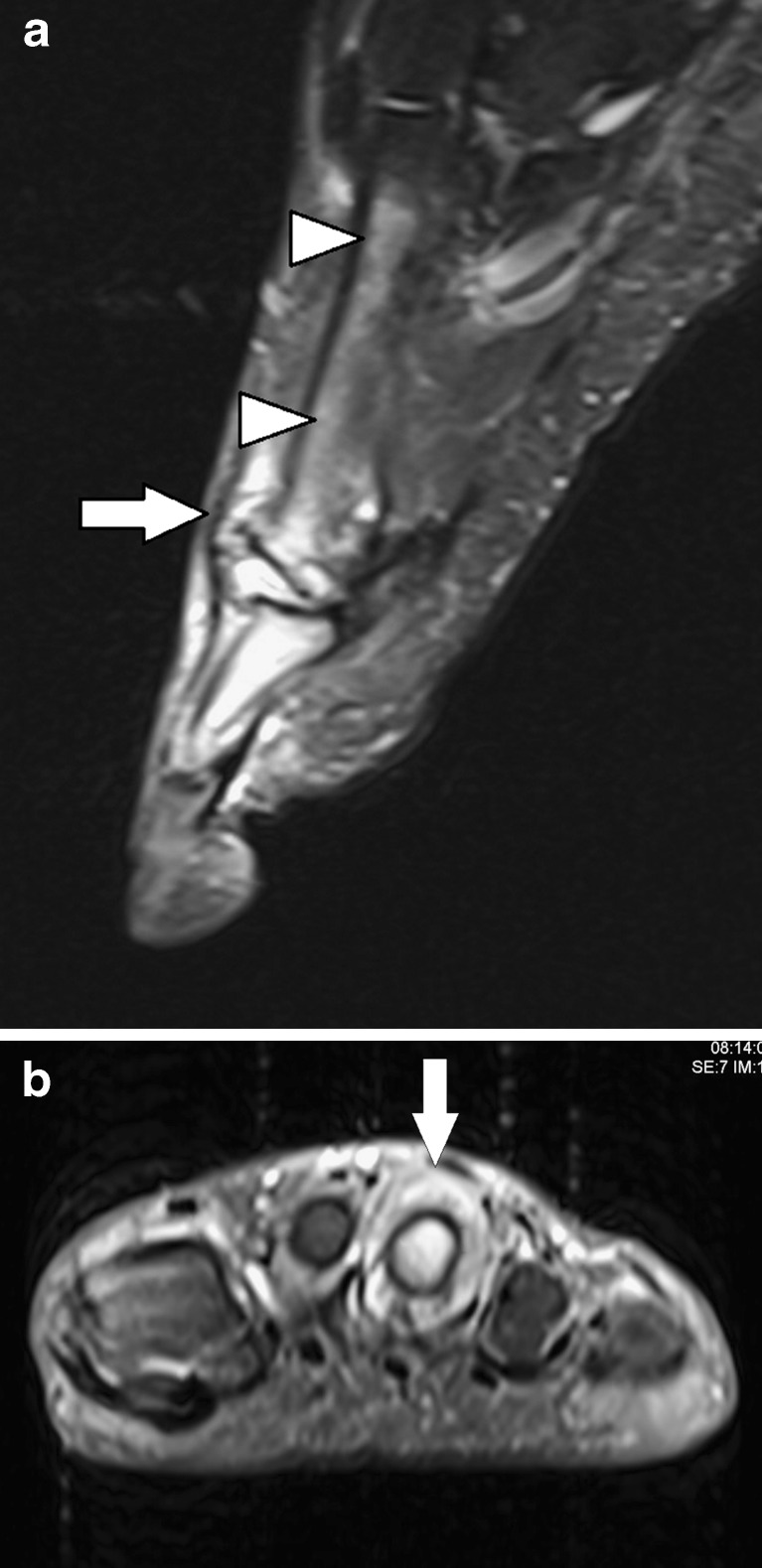
Morton’s neuroma (fibroma). Short-axis T1-WI (a), T2-WI (b) and fat-suppressed contrast-enhanced T1-WI (c): spindle-shaped lesion at the third intermetatarsal space (short arrow), located plantar to the deep transverse intermetatarsal ligament, with low SI on T1-WI and T2-WI. Overestimation in size on T1-WI due to associated (hypointense) fluid in the intermetatarsal bursa (long arrow), revealed as hyperintense on T2-WI. There is moderate contrast enhancement of the fibroma, as well as some rim enhancement of the bursa
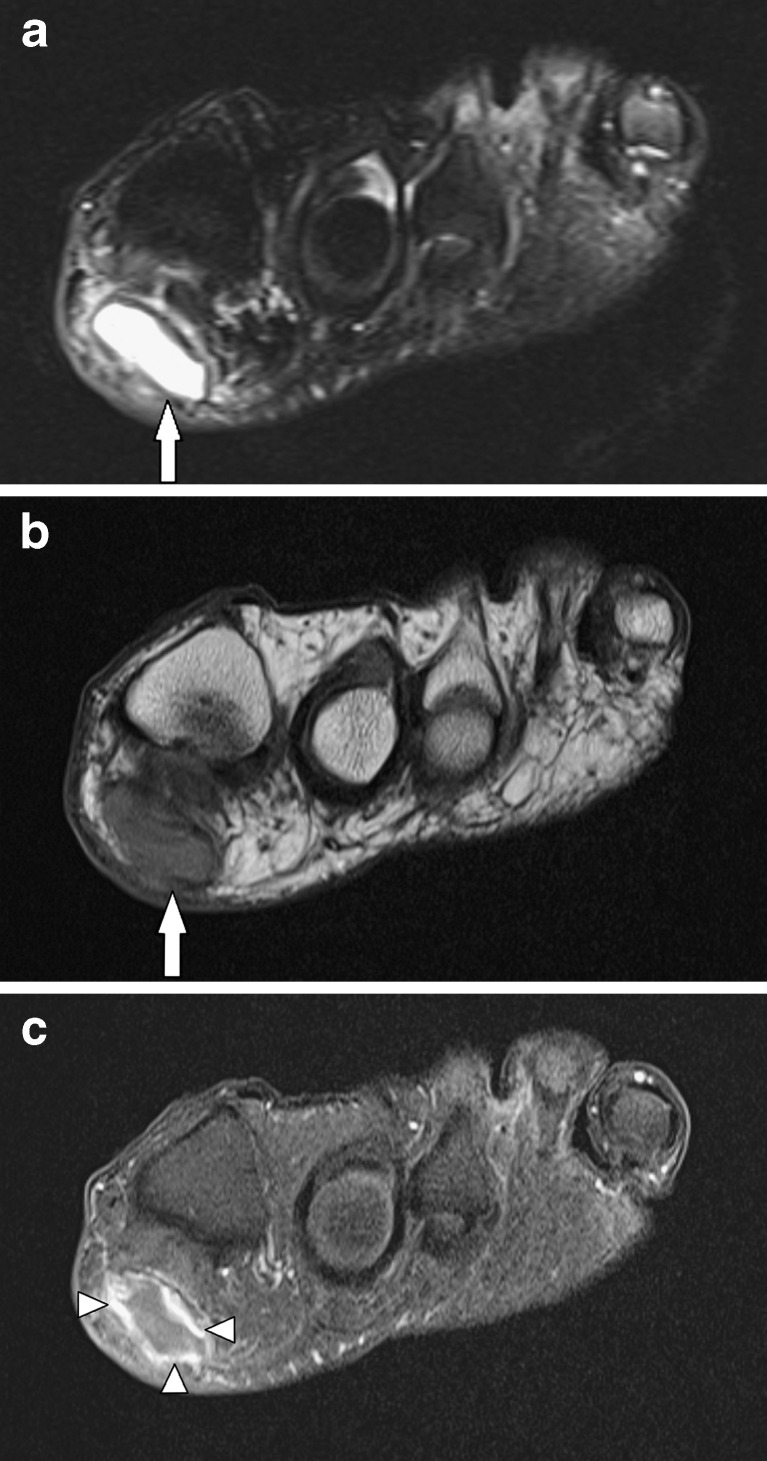
Adventitious bursitis. A 54-year-old patient with a painful swelling located plantar to the first metatarsophalangeal joint. Short-axis fat-suppressed T2-WI (a), T1-WI (b) and fat-suppressed contrast-enhanced T1-WI (c): fluid collection plantar-medial to the first metatarsal head (long arrow) of high SI on T2-WI, and low SI on T1-WI, corresponding to a fluid-filled cavity. There is marked rim enhancement (arrowheads)
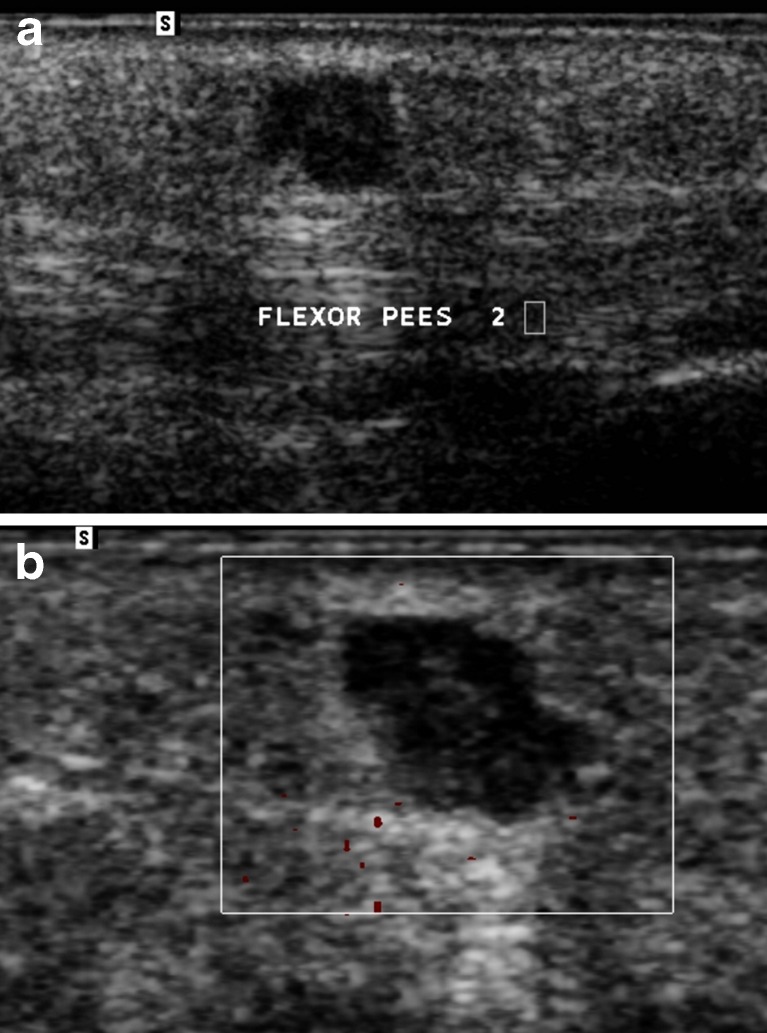
Ultrasound of epidermoid cyst on the sole of the foot. The ultrasound images demonstrate a hypoechogenic polylobular lesion with posterior acoustic enhancement containing some scattered echogenic reflective material. The cyst is located in the subcutaneous fat superficial to the flexor tendon of the second digit
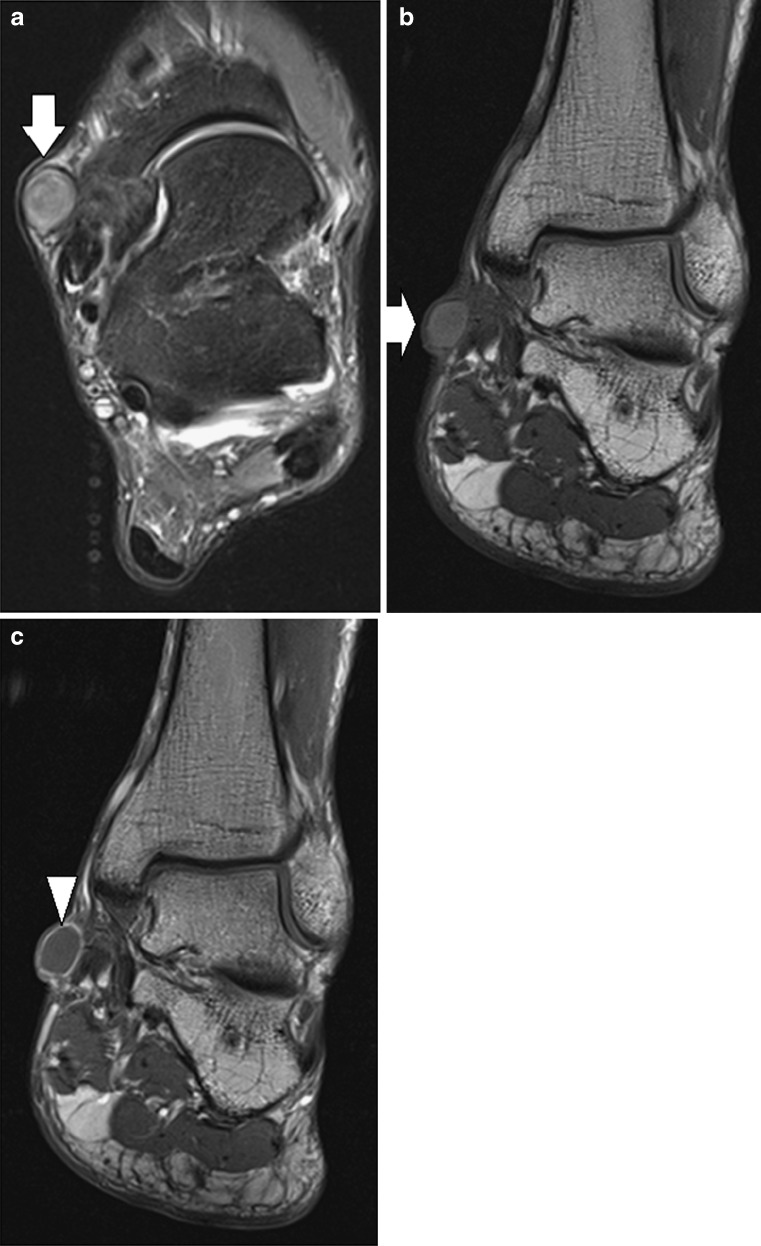
Epidermoid cyst (different patient from that in Fig. 7). Axial fat-suppressed T2-WI (a), coronal T1-WI (b) and coronal contrast-enhanced T1-WI (c). Unilocular, well-defined subcutaneous lesion (arrows) at the medial aspect of the ankle. The lesion has intermediate SI on T2-WI with some small areas of lower SI (probably due to keratinous debris), and is slightly hyperintense to muscle on T1-WI. A peripheral rim enhancement is seen (arrowhead), without internal enhancement
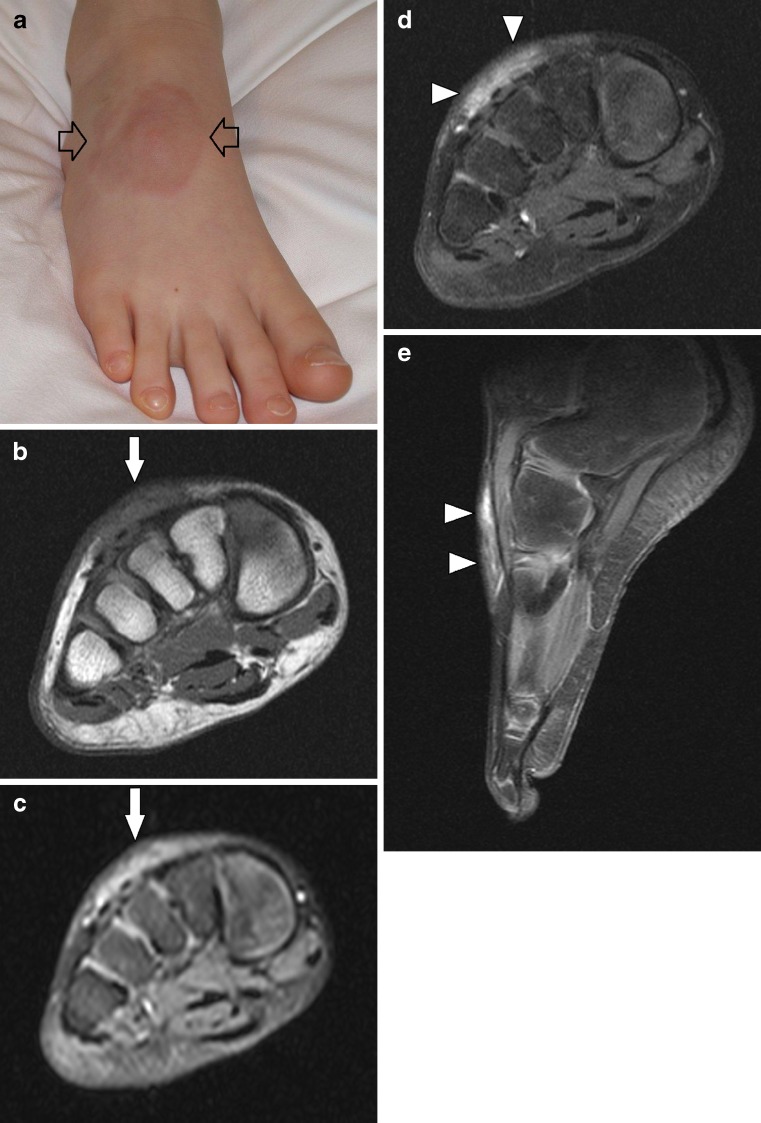
Granuloma annulare (combined cutaneous-subcutaneous presentation). A 14-year-old patient presenting with a round, erythematous skin lesion at the dorsum of the foot (a), with mild associated swelling. MR images: short axis T1-WI (b) and fat-suppressed T2-WI (c); short-axis (d) and sagittal (e) fat-suppressed contrast-enhanced T1-WI. Disc-like, ill-defined subcutaneous lesion at the dorsum of the foot. The lesion is iso-intense to muscle on T1-WI, is of high SI on T2-WI and demonstrates marked, slightly heterogeneous contrast enhancement
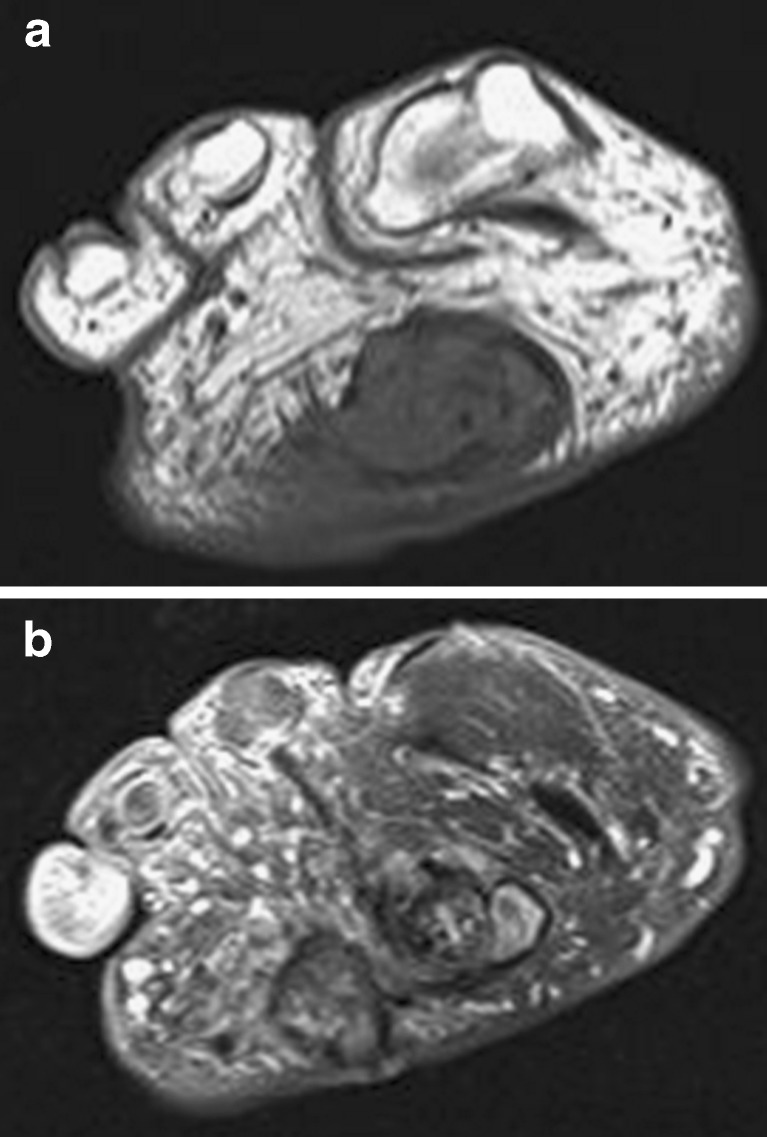
Rheumatoid nodule. Short-axis T1-WI (a), fat-suppressed T2-WI (b): nodular lesion at the plantar subcutaneous fat tissue at the level of the metatarsals. The lesion is of low SI on T1-WI, whereas heterogeneity is seen on T2-WI. Multiple erosions were seen at the metatarsophalangeal joints (not shown)

Tenosynovitis of the flexor hallucis longus (FHL). Sagittal T1-WI (a) and long-axis T2-WI (b): there is marked effusion (short arrow) in the tendon sheath of the FHL (long arrow), of low SI on T1-WI and high SI on T2-WI
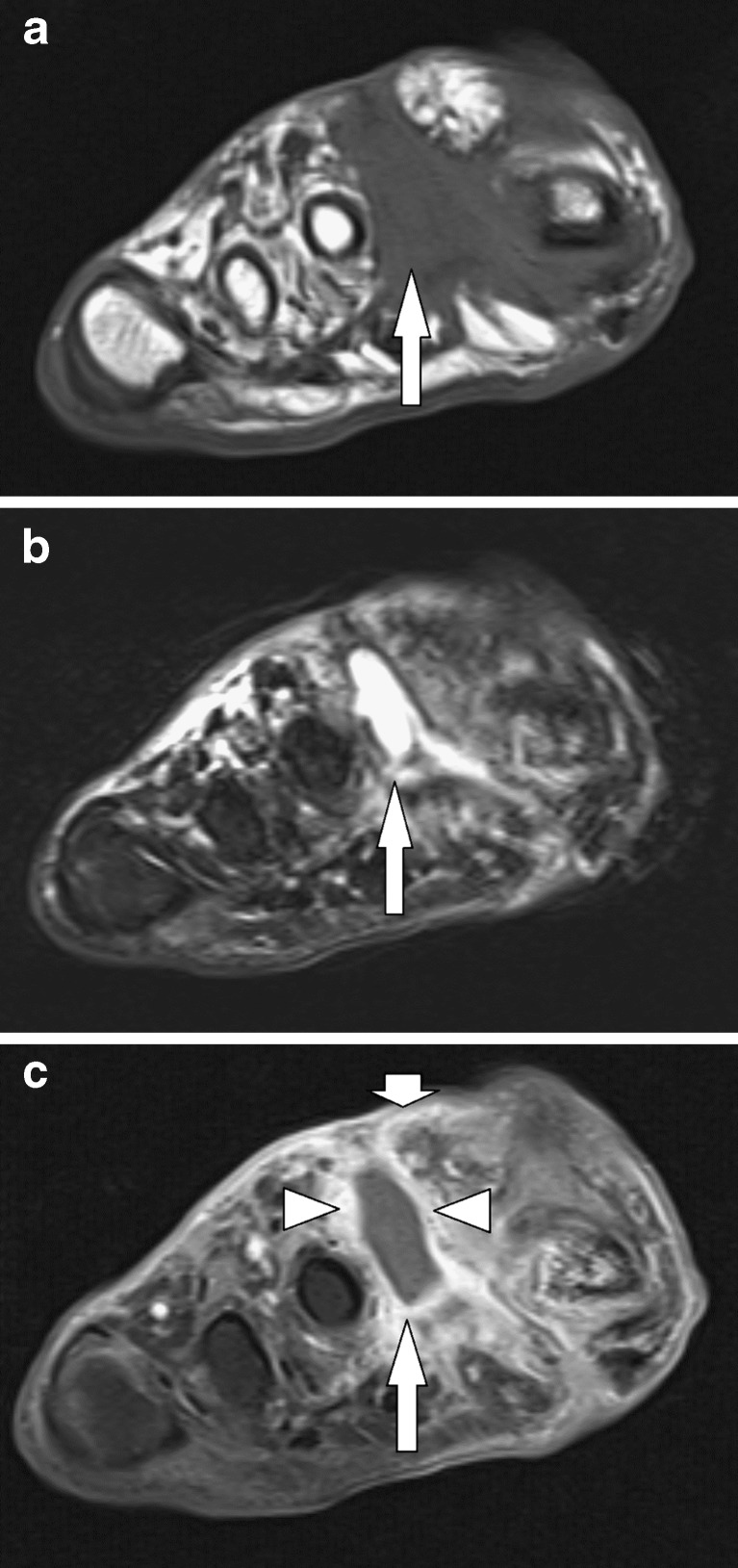
Abscess. A 50-year-old diabetic patient, 2 years after amputation of the second digit (including the metatarsal head), presenting with a painless swelling at the region of previous surgery. Short-axis T1-WI (a), fat-suppressed T2-WI (b) and fat-suppressed contrast-enhanced T1-WI (c) demonstrate a collection (long arrow) in the soft tissue between the first and second metatarsal heads, of low SI on T1-WI, high SI on T2-WI and thick rim enhancement (arrowheads). There is increased SI on T2-WI of the adjacent soft tissue and dermis as well as contrast enhancement, corresponding to oedema and cellulitis (short arrow)

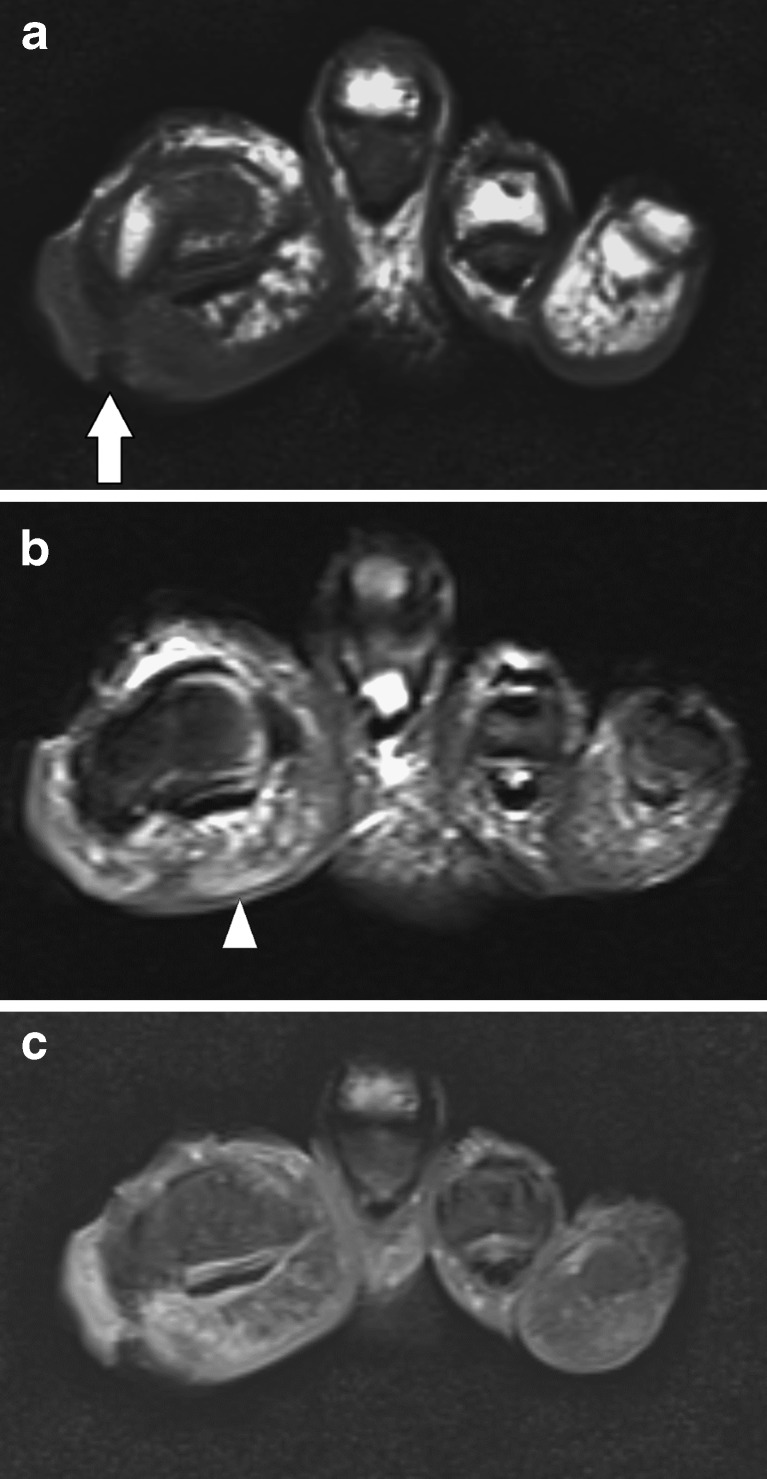
Tophaceus gout. Short-axis T1-WI (a), sagittal fat-suppressed T2-WI (b) and short-axis fat-suppressed contrast-enhanced T1-WI (c): The gouty tophus (short arrows) is isointense to muscle on T1-WI and of heterogeneous SI on T2-WI. The lesion displays heterogeneous enhancement (arrowheads). There is evidence of erosive joint disease at the metatarsophalangeal joints (long arrows)
Diabetic callus. Short-axis T1-WI (a), fat-suppressed T2-WI (b) and fat-suppressed contrast-enhanced T1-WI (c): callus with central ulceration (arrow) in the subcutaneous fat medial and plantar to the first metatarsal head, with low SI on T1-WI, intermediate SI on T2-WI and heterogeneous contrast enhancement. There is some oedema in the adjacent fat (arrowhead)
Periosteal callus secondary to Freiberg’s infraction. Sagittal (a) and short-axis (b) fat-suppressed T2-WI demonstrates flattening and deformation of the head of the second metatarsal bone with prominent periosteal callus formation (arrow) and bone marrow oedema (arrowheads)
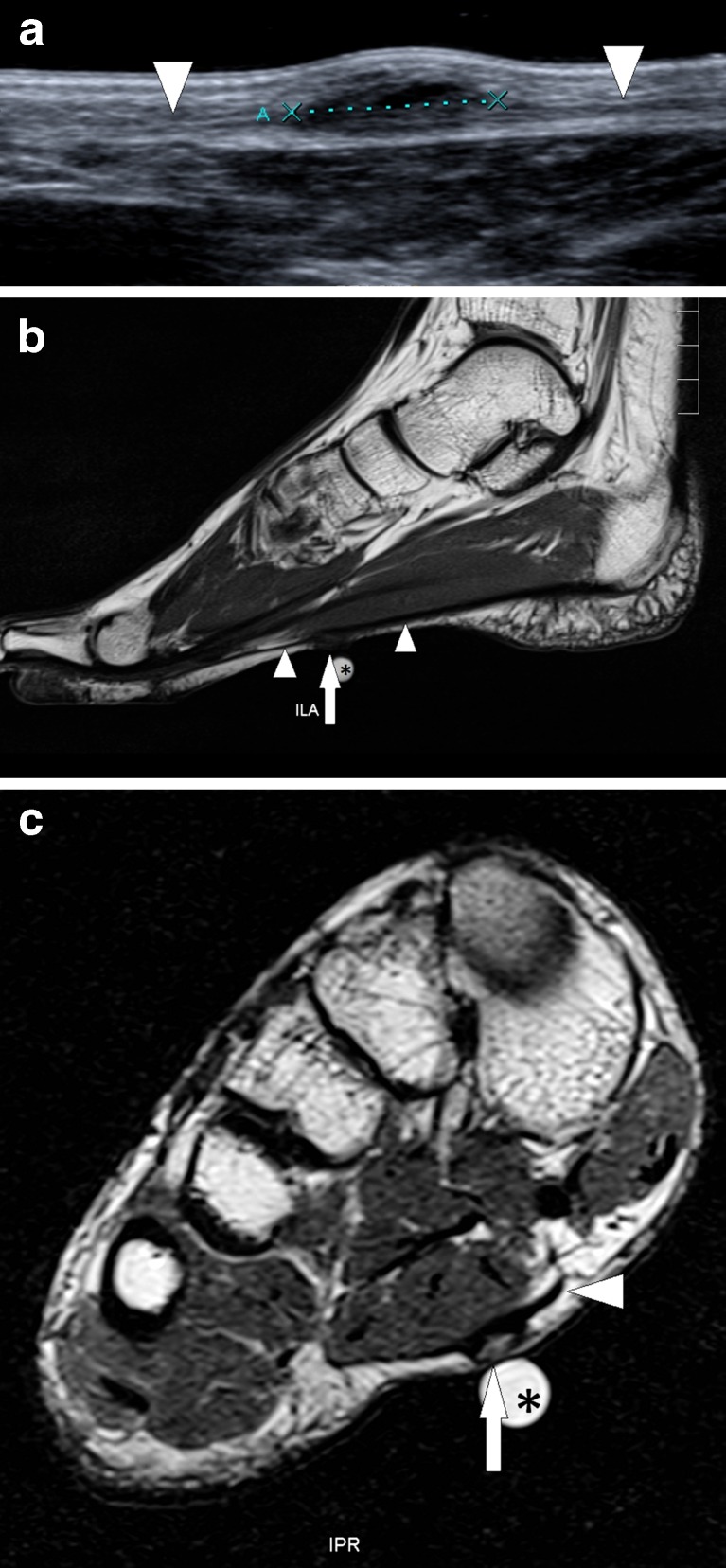
Plantar fibromatosis. Patient with a painless subcutaneous nodule at the medial aspect of the foot sole. Ultrasound image (a) along the sagittal plane displays a hypo-echogenic ill-defined lesion at the medial bundle of the plantar aponeurosis, with a length of 11 mm. Long-axis T1-WI (b) and short-axis T2-WI (c) clearly demonstrate the relationship between the lesion (arrow) and the plantar aponeurosis (arrowheads). The fibromatosis is iso-intense to muscle on T1-WI and slightly hyperintense on T2-WI. The nodular extracorporeal structure (asterisk) is an imaging marker placed on the skin for easy lesion localisation
References
-
- Kinoshita M, Okuda R, Morikawa J, Abe M. Tarsal tunnel syndrome associated with an accessory muscle. Foot Ankle Int. 2003;24:132–136. - PubMed
-
- Vanhoenacker FM, Perre S, Vuyst D, Schepper AM. Cystic lesions around the knee. JBR BTR. 2003;86(5):302–304. - PubMed
-
- Kliman ME, Freiberg A. Ganglia of the foot and ankle. Foot Ankle. 1982;3(1):45–46. - PubMed
LinkOut - more resources
Full Text Sources