

Imaging of breast implants-a pictorial review
- PMID: 22347984
- PMCID: PMC3259319
- DOI: 10.1007/s13244-011-0122-3
Imaging of breast implants-a pictorial review
Abstract
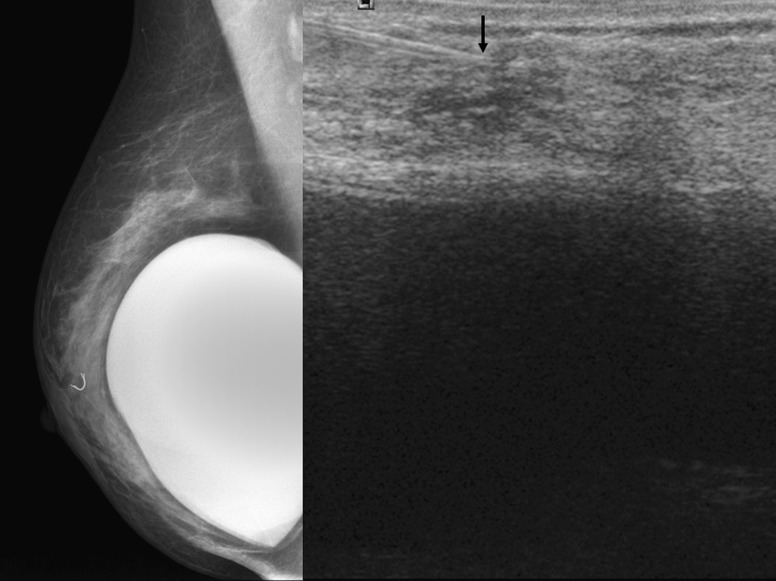
The number of women with breast implants is increasing. Radiologists must be familiar with the normal and abnormal findings of common implants. Implant rupture is a well-known complication after surgery and is the main cause of implant removal. Although mammography and ultrasonography are the standard first steps in the diagnostic workup, magnetic resonance imaging (MRI) is the most useful imaging modality for the characterisation of breast implants because of its high spatial resolution and contrast between implants and soft tissues and absence of ionising radiation. MRI has the highest sensitivity and specificity for implant rupture, thanks to its sequences that can suppress or emphasise the signal from silicone. Regardless of the technique used, the overall aim of imaging breast implants is to provide essential information about tissue and prosthesis integrity, detect implant abnormalities and detect breast diseases unrelated to implants, such as breast cancer.
Figures


References
LinkOut - more resources
Full Text Sources
Other Literature Sources