

Causes and imaging features of false positives and false negatives on F-PET/CT in oncologic imaging
- PMID: 22347986
- PMCID: PMC3259390
- DOI: 10.1007/s13244-010-0062-3
Causes and imaging features of false positives and false negatives on F-PET/CT in oncologic imaging
Abstract
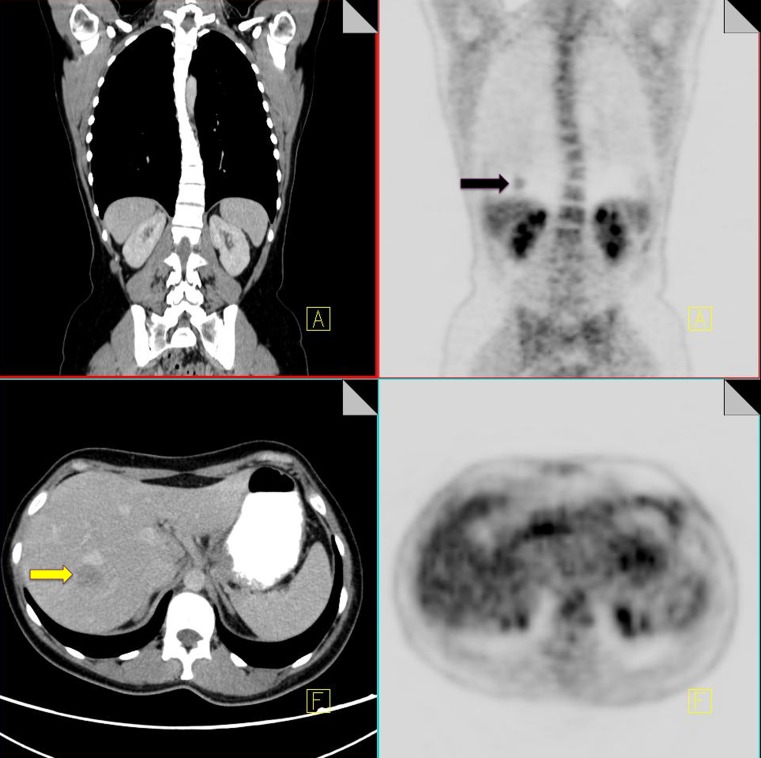
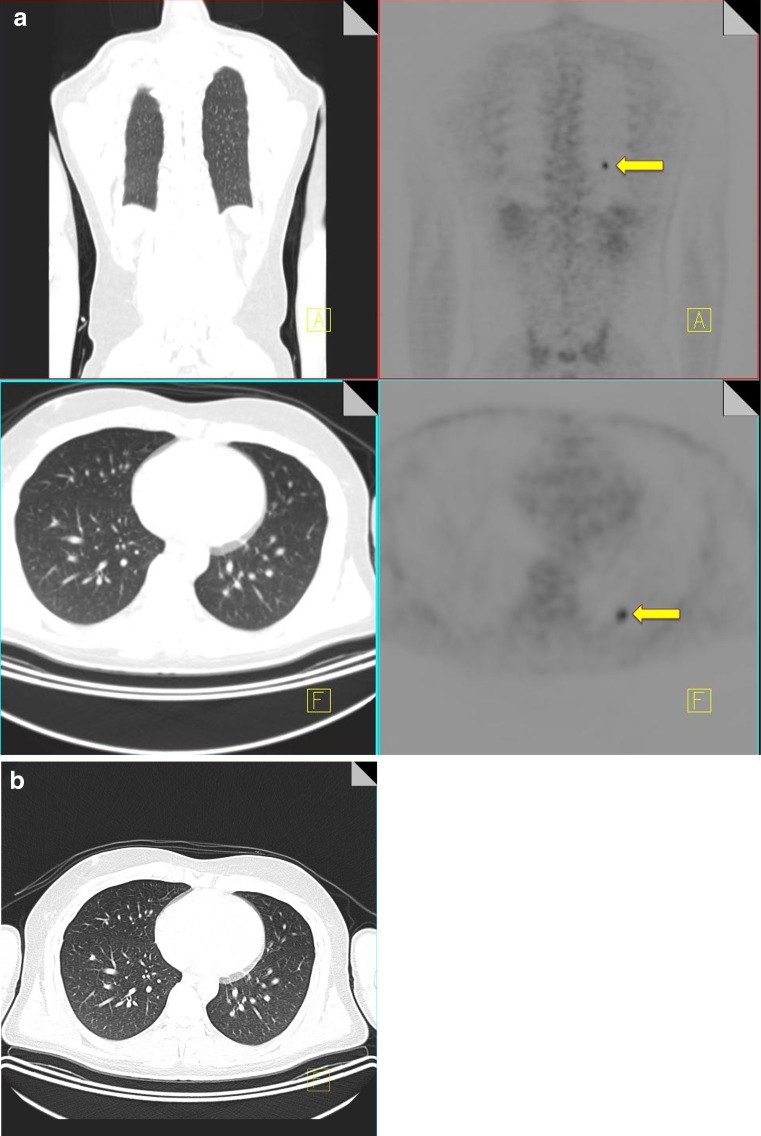
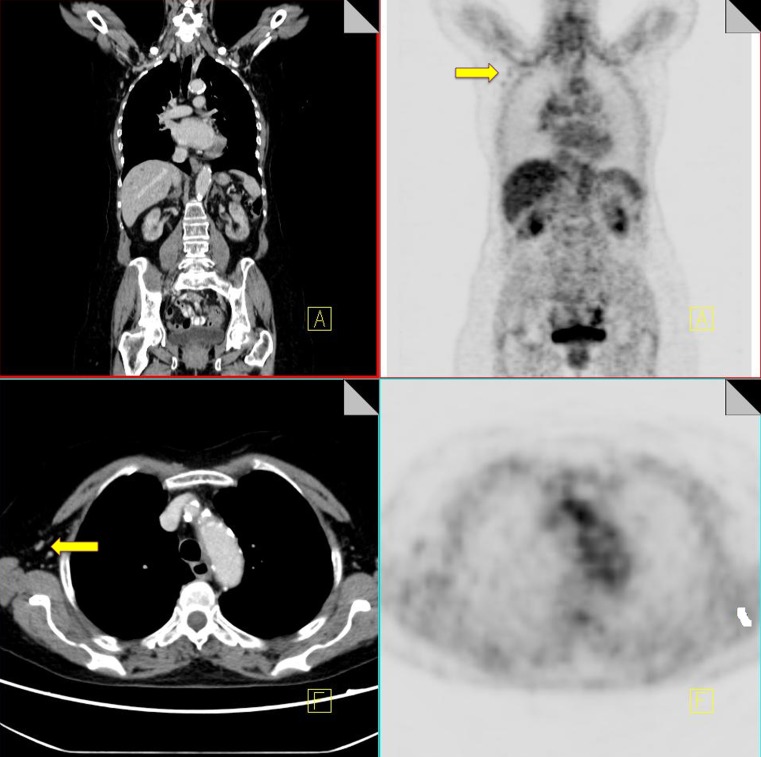
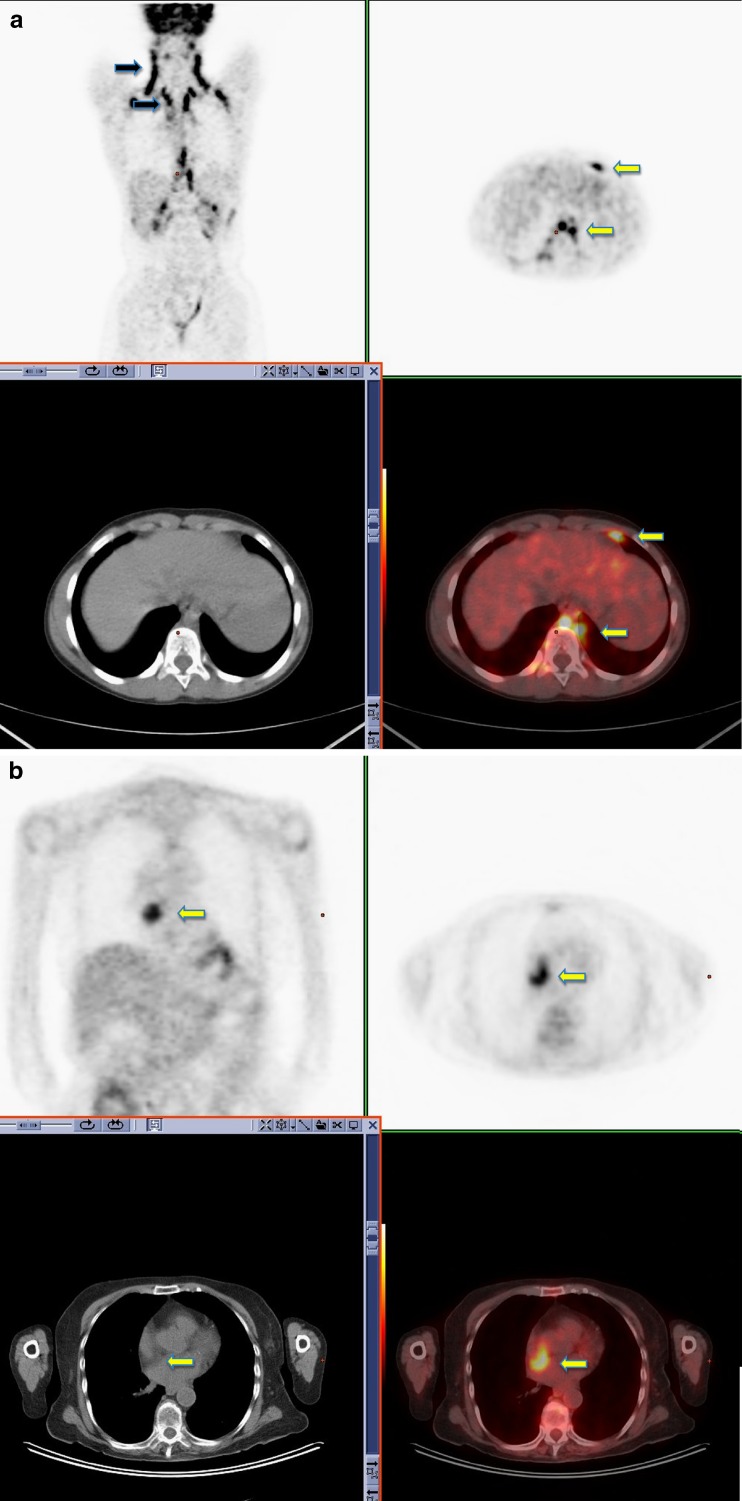
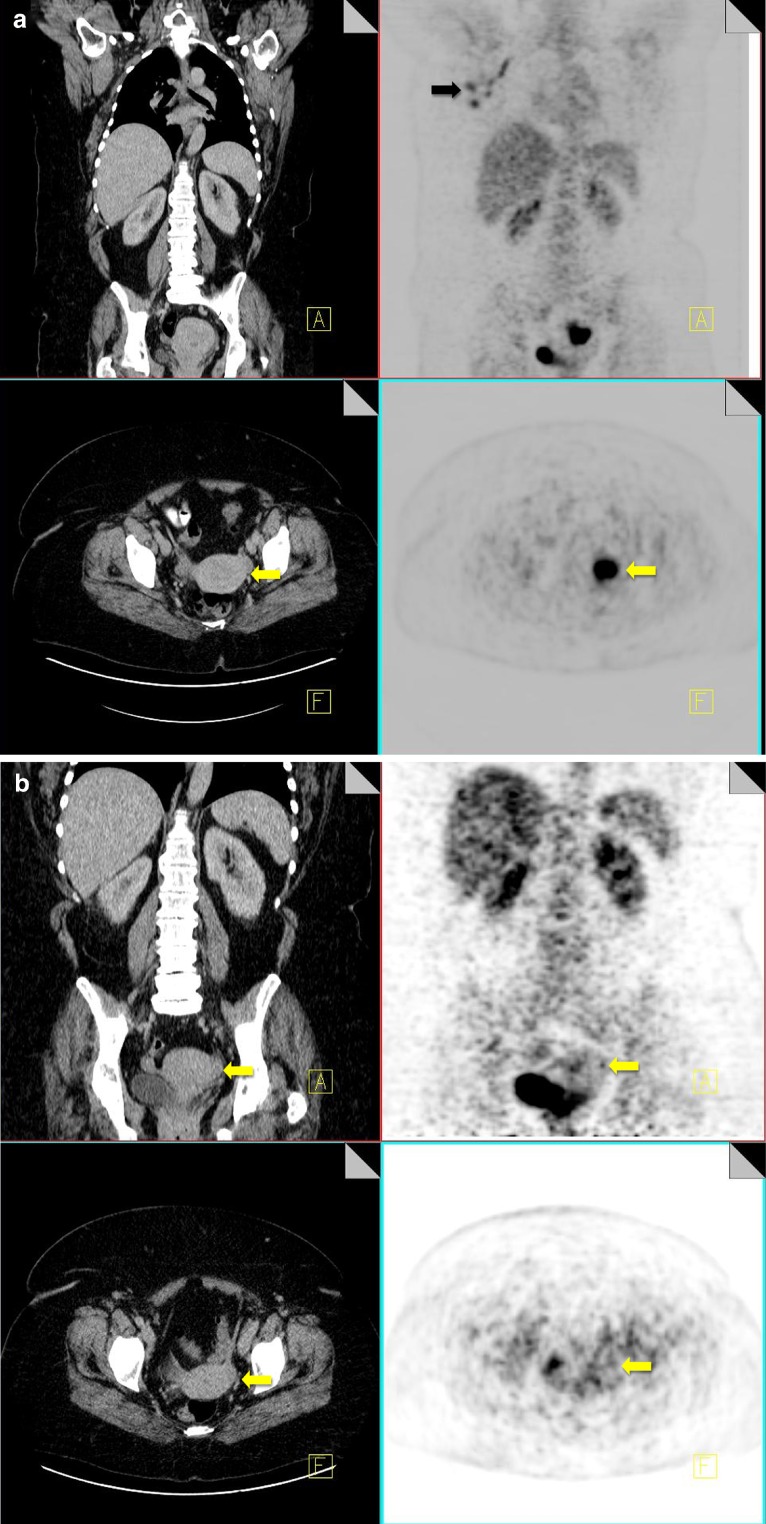
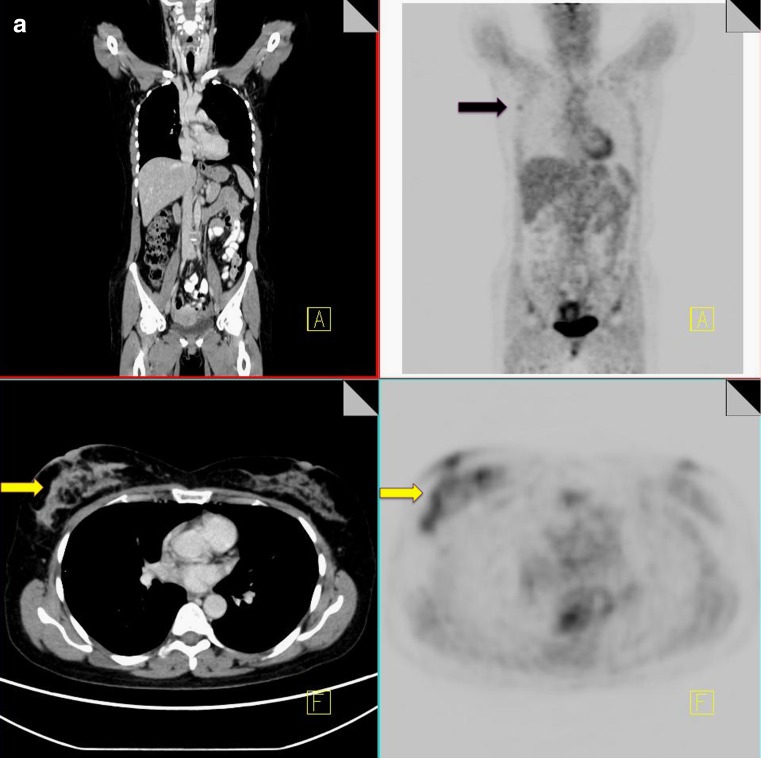
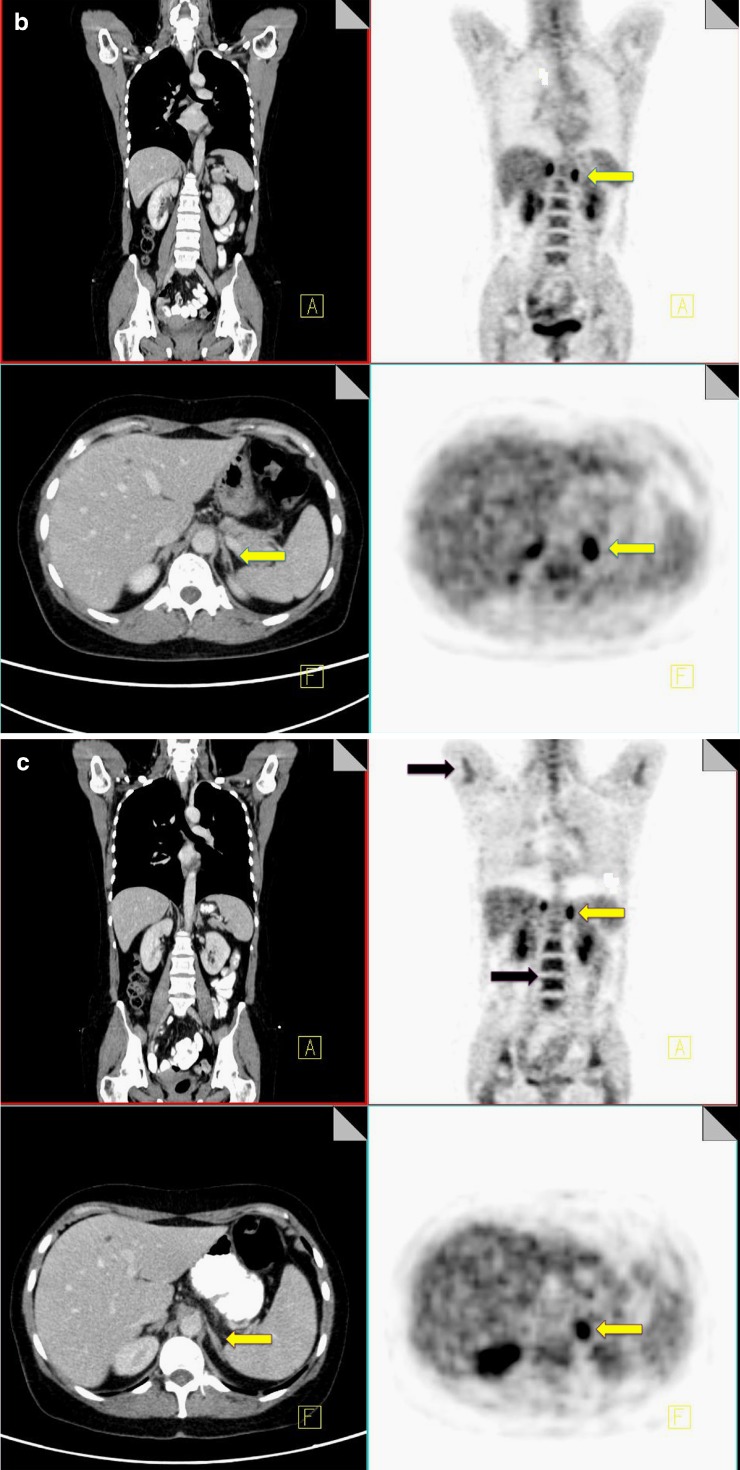
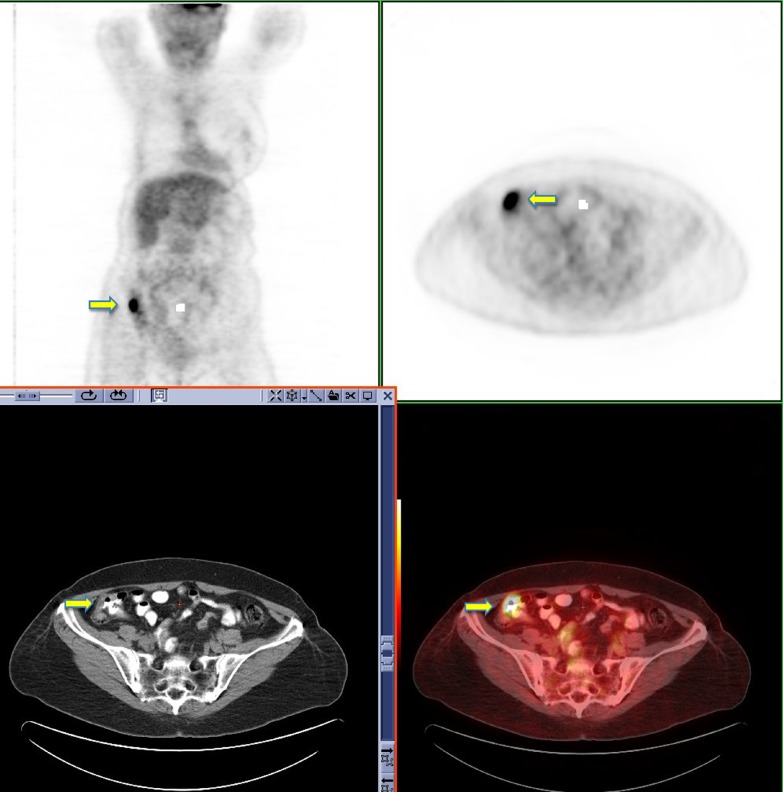
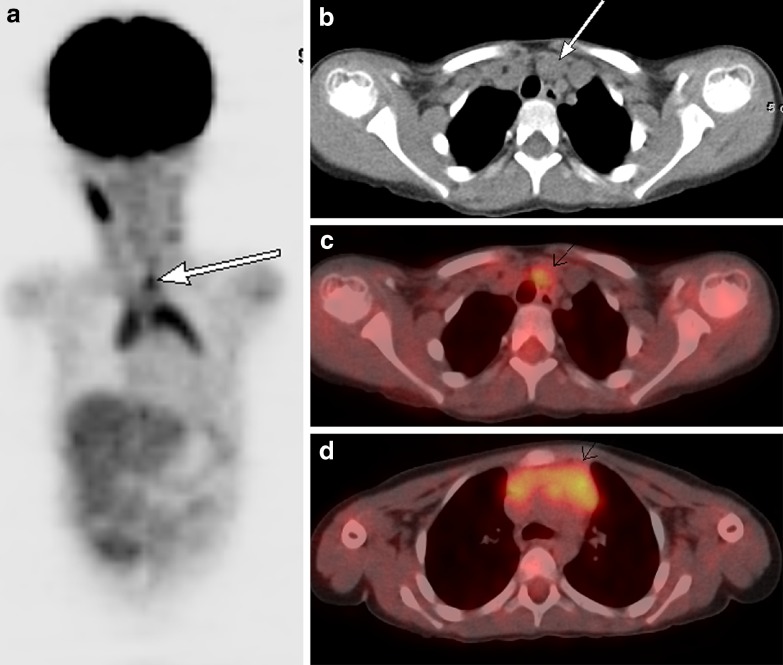
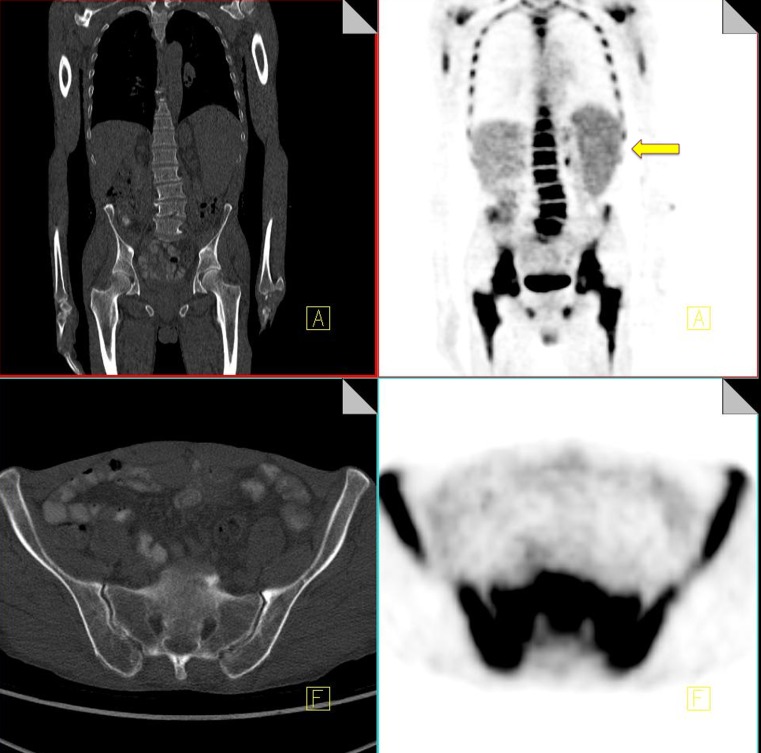
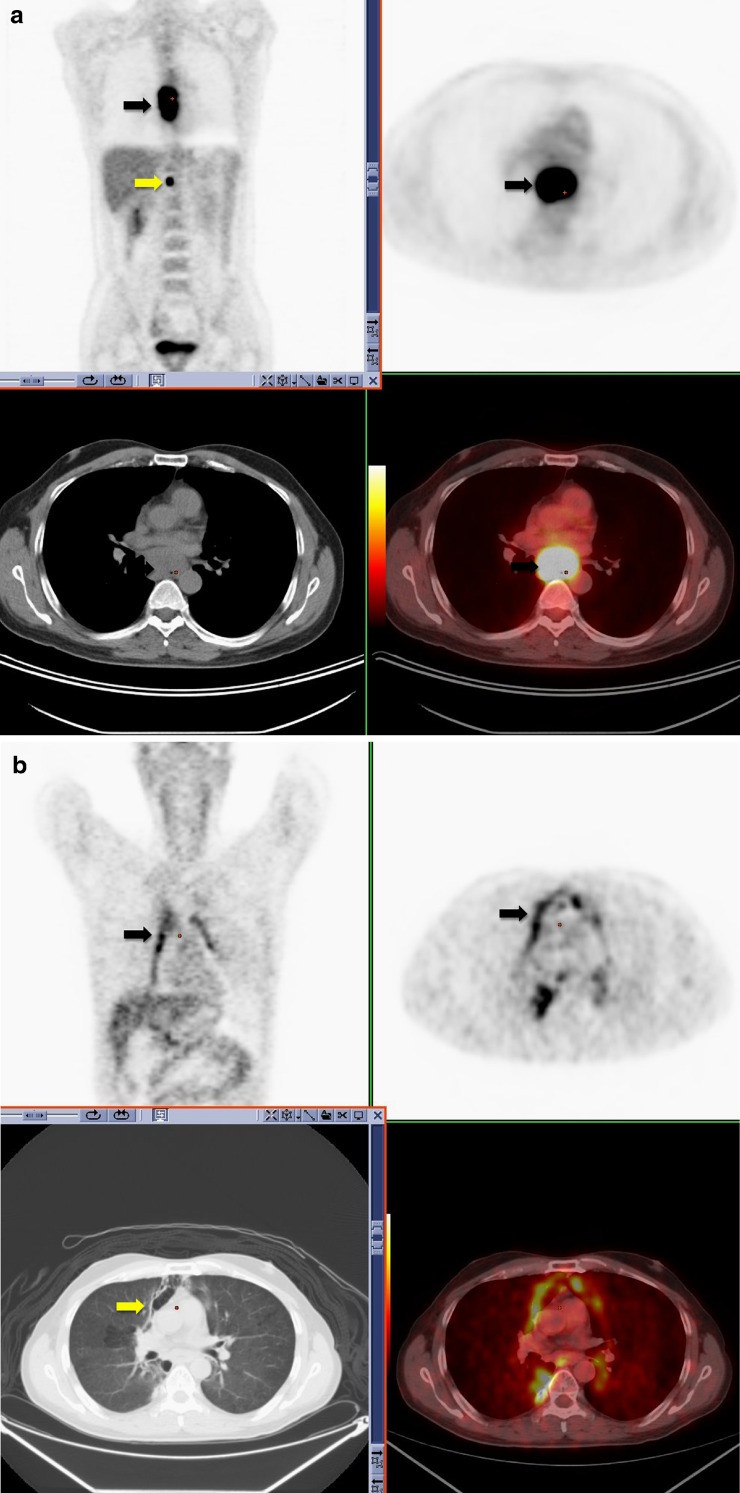
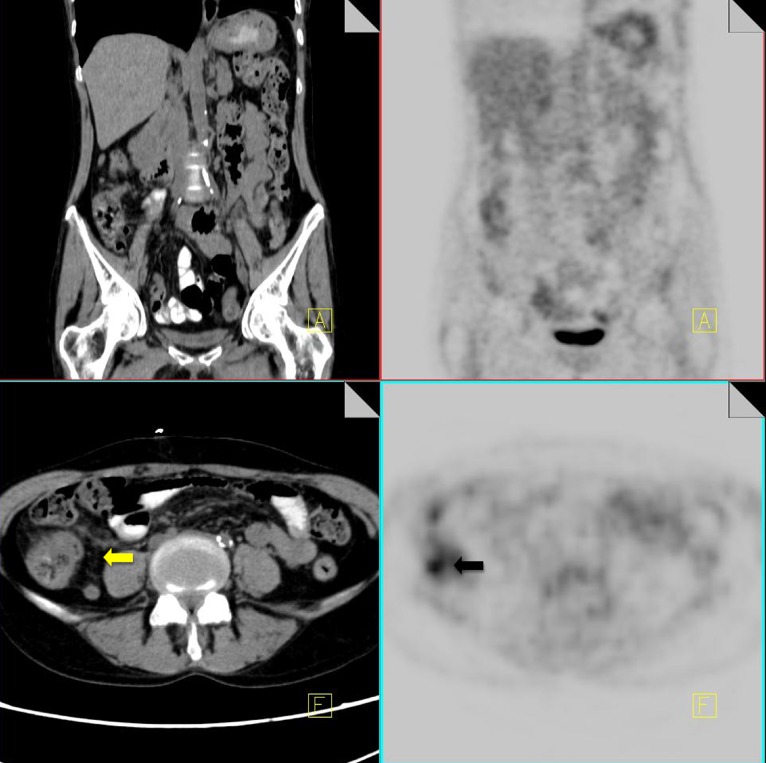
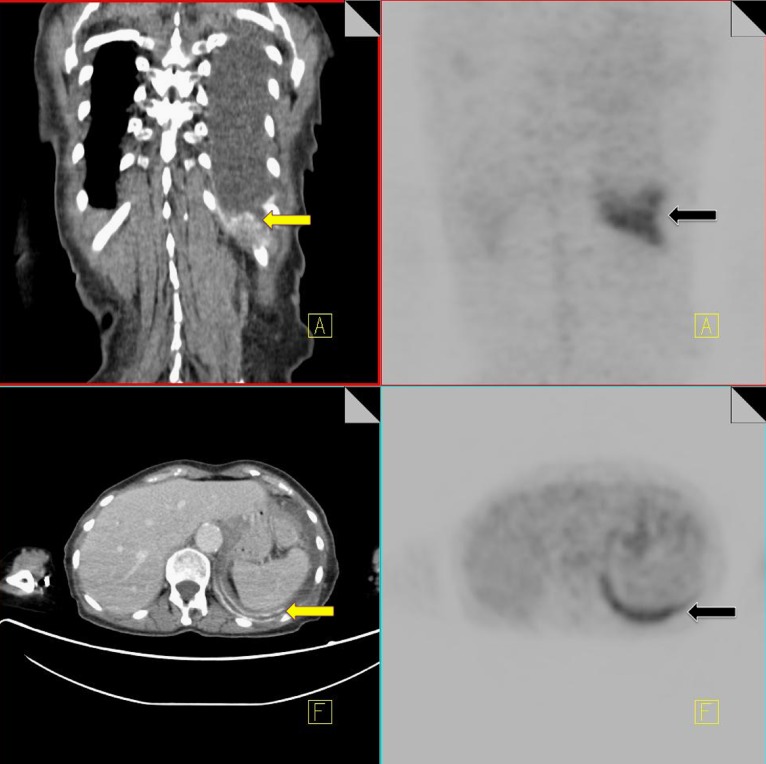
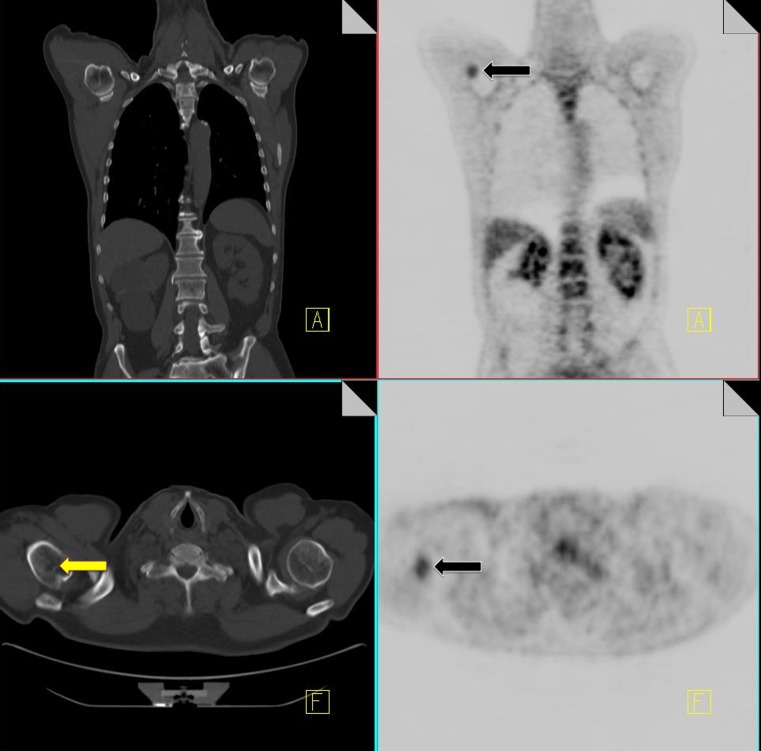
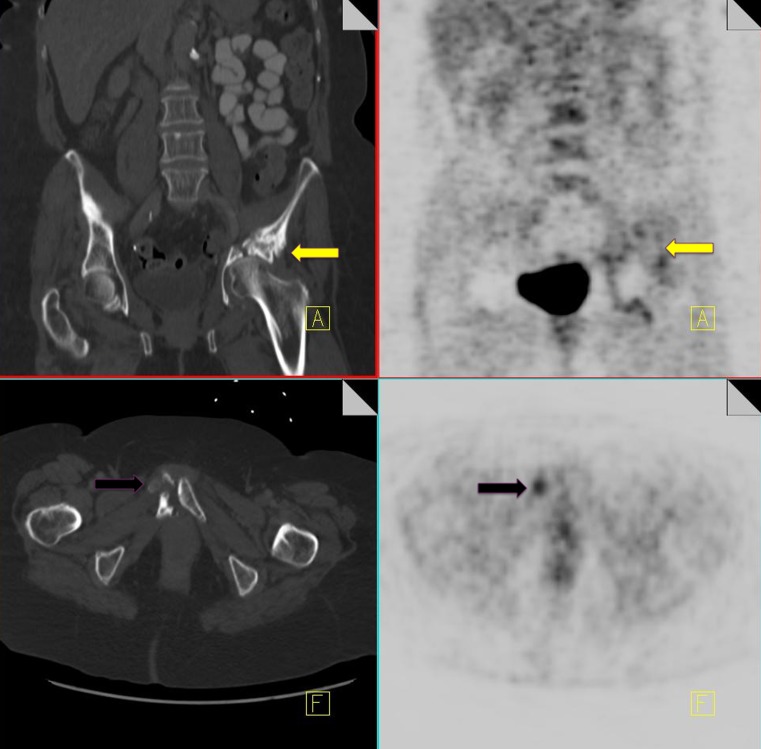
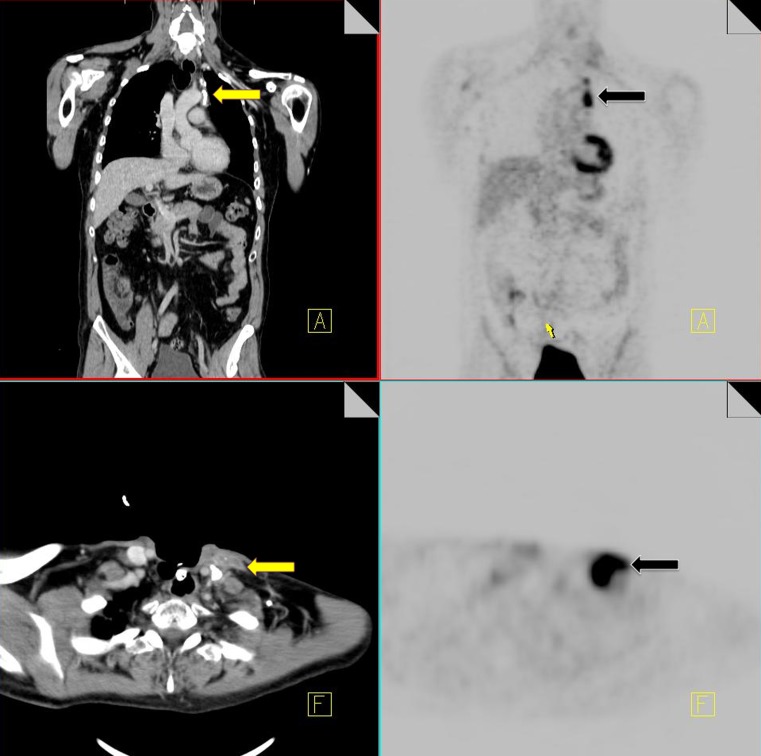
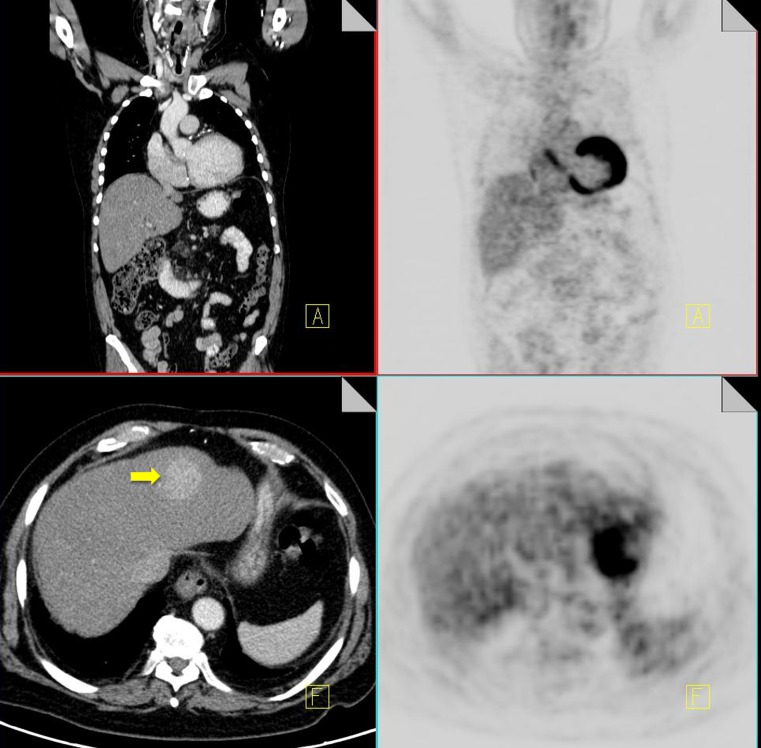
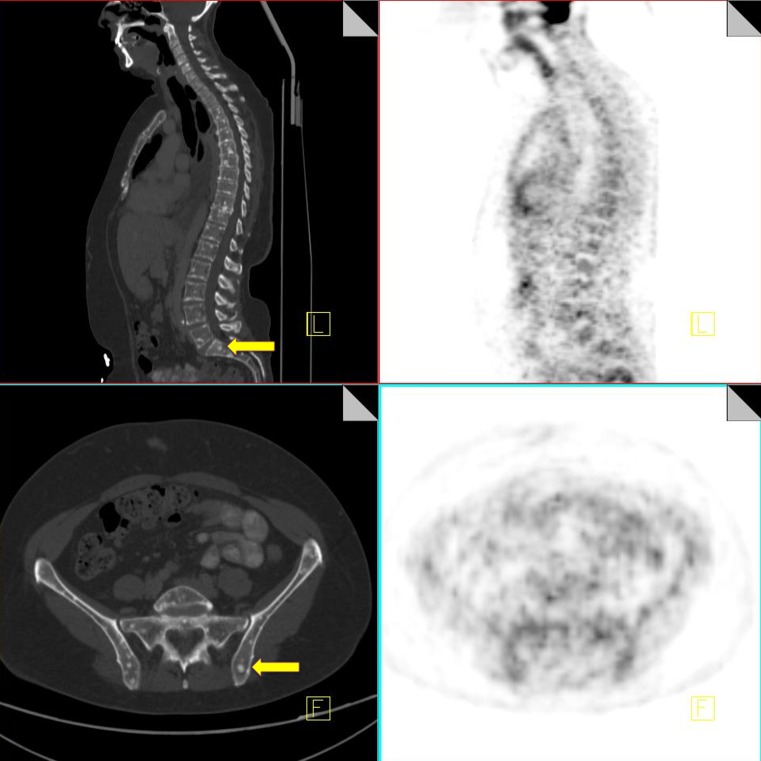
BACKGROUND: 18F-FDG is a glucose analogue that is taken up by a wide range of malignancies. 18F-FDG PET-CT is now firmly established as an accurate method for the staging and restaging of various cancers. However, 18F-FDG also accumulates in normal tissue and other non-malignant conditions, and some malignancies do not take up F18-FDG or have a low affinity for the tracer, leading to false-positive and false-negative interpretations. METHODS: PET-CT allows for the correlation of two separate imaging modalities, combining both morphological and metabolic information. We should use the CT to help interpret the PET findings. In this article we will highlight specific false-negative and false-positive findings that one should be aware of when interpreting oncology scans. RESULTS: We aim to highlight post-treatment conditions that are encountered routinely on restaging scans that can lead to false-positive interpretations. We will emphasise the importance of using the CT component to help recognise these entities to allow improved diagnostic accuracy. CONCLUSION: In light of the increased use of PET-CT, it is important that nuclear medicine physicians and radiologists be aware of these conditions and correlate the PET and CT components to avoid misdiagnosis, over staging of disease and unnecessary biopsies.
Figures
References
-
- Wahl RL. Targeting glucose transporters for tumor imaging: “sweet” idea, “sour” result. J Nucl Med. 1996;37(6):1038–1041. - PubMed
-
- Kim BT, Kim Y, Lee KS, Yoon SB, Cheon EM, Kwon OJ, Rhee CH, Han J, Shin MH. Localized form of bronchioalveolar carcinoma: FDG PET findings. AJR. 1998;170(4):935–939. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources