

Interventions to reduce medication errors in adult intensive care: a systematic review
- PMID: 22348303
- PMCID: PMC3477343
- DOI: 10.1111/j.1365-2125.2012.04220.x
Interventions to reduce medication errors in adult intensive care: a systematic review
Abstract
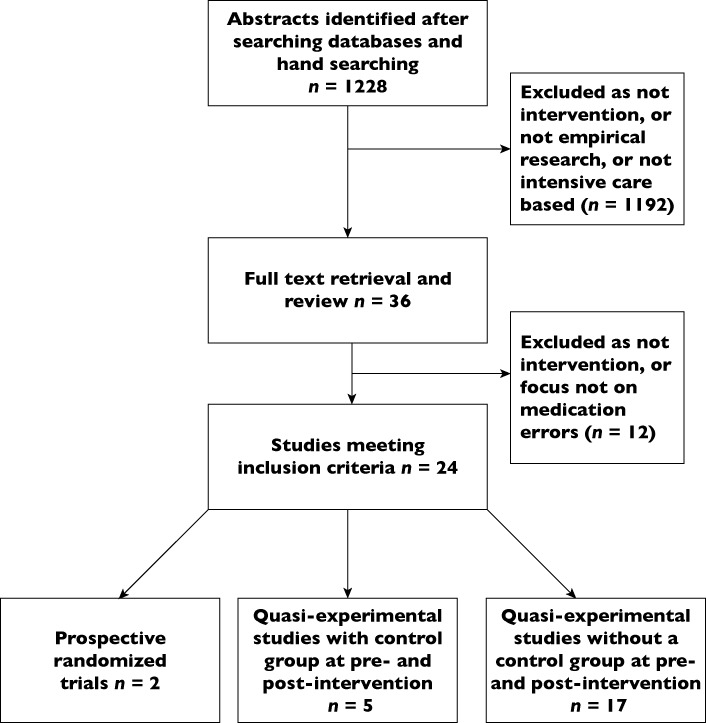
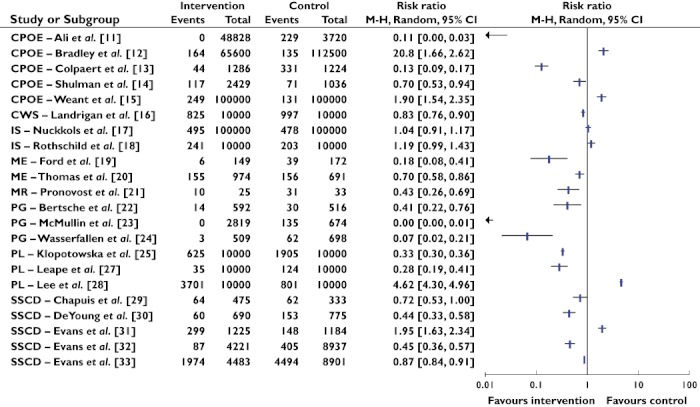
Critically ill patients need life saving treatments and are often exposed to medications requiring careful titration. The aim of this paper was to review systematically the research literature on the efficacy of interventions in reducing medication errors in intensive care. A search was conducted of PubMed, CINAHL EMBASE, Journals@Ovid, International Pharmaceutical Abstract Series via Ovid, ScienceDirect, Scopus, Web of Science, PsycInfo and The Cochrane Collaboration from inception to October 2011. Research studies involving delivery of an intervention in intensive care for adult patients with the aim of reducing medication errors were examined. Eight types of interventions were identified: computerized physician order entry (CPOE), changes in work schedules (CWS), intravenous systems (IS), modes of education (ME), medication reconciliation (MR), pharmacist involvement (PI), protocols and guidelines (PG) and support systems for clinical decision making (SSCD). Sixteen out of the 24 studies showed reduced medication error rates. Four intervention types demonstrated reduced medication errors post-intervention: CWS, ME, MR and PG. It is not possible to promote any interventions as positive models for reducing medication errors. Insufficient research was undertaken with any particular type of intervention, and there were concerns regarding the level of evidence and quality of research. Most studies involved single arm, before and after designs without a comparative control group. Future researchers should address gaps identified in single faceted interventions and gather data on multi-faceted interventions using high quality research designs. The findings demonstrate implications for policy makers and clinicians in adopting resource intensive processes and technologies, which offer little evidence to support their efficacy.
© 2012 The Authors. British Journal of Clinical Pharmacology © 2012 The British Pharmacological Society.
Figures
Similar articles
-
Reducing medication errors for adults in hospital settings.Cochrane Database Syst Rev. 2021 Nov 25;11(11):CD009985. doi: 10.1002/14651858.CD009985.pub2. Cochrane Database Syst Rev. 2021. PMID: 34822165 Free PMC article.
-
Professional, structural and organisational interventions in primary care for reducing medication errors.Cochrane Database Syst Rev. 2017 Oct 4;10(10):CD003942. doi: 10.1002/14651858.CD003942.pub3. Cochrane Database Syst Rev. 2017. PMID: 28977687 Free PMC article.
-
The effectiveness of interventions to meet family needs of critically ill patients in an adult intensive care unit: a systematic review update.JBI Database System Rev Implement Rep. 2016 Mar;14(3):181-234. doi: 10.11124/JBISRIR-2016-2477. JBI Database System Rev Implement Rep. 2016. PMID: 27532144
-
Antidepressants for pain management in adults with chronic pain: a network meta-analysis.Health Technol Assess. 2024 Oct;28(62):1-155. doi: 10.3310/MKRT2948. Health Technol Assess. 2024. PMID: 39367772 Free PMC article.
-
Interventions for interpersonal communication about end of life care between health practitioners and affected people.Cochrane Database Syst Rev. 2022 Jul 8;7(7):CD013116. doi: 10.1002/14651858.CD013116.pub2. Cochrane Database Syst Rev. 2022. PMID: 35802350 Free PMC article.
Cited by
-
The effect of the TIM program (Transfer ICU Medication reconciliation) on medication transfer errors in two Dutch intensive care units: design of a prospective 8-month observational study with a before and after period.BMC Health Serv Res. 2017 Feb 10;17(1):124. doi: 10.1186/s12913-017-2065-y. BMC Health Serv Res. 2017. PMID: 28183302 Free PMC article.
-
Medication errors in neonatal intensive care unit of a tertiary care hospital in South India: A prospective observational study.Indian J Pharmacol. 2020 Jul-Aug;52(4):260-265. doi: 10.4103/ijp.IJP_611_19. Indian J Pharmacol. 2020. PMID: 33078726 Free PMC article.
-
Pharmacist-led educational interventions provided to healthcare providers to reduce medication errors: A systematic review and meta-analysis.PLoS One. 2021 Jun 23;16(6):e0253588. doi: 10.1371/journal.pone.0253588. eCollection 2021. PLoS One. 2021. PMID: 34161388 Free PMC article.
-
Pharmacoeconomic effect of compliance with pharmacist's intervention based on cancer chemotherapy regimens: a cohort study.J Pharm Health Care Sci. 2015 Mar 5;1:10. doi: 10.1186/s40780-014-0007-y. eCollection 2015. J Pharm Health Care Sci. 2015. PMID: 26819721 Free PMC article.
-
Perfusions continues et pompes intelligentes en néonatologie : une analyse « pré-post » des modes de défaillance, de leurs effets et de leur criticité (AMDEC).Can J Hosp Pharm. 2015 Sep-Oct;68(5):406-11. Can J Hosp Pharm. 2015. PMID: 26478587 Free PMC article. French. No abstract available.
References
-
- Kiekkas P, Karga M, Lemonidou C, Aretha D, Karanikolas M. Medication errors in critically ill adults: a review of direct observation evidence. Am J Crit Care. 2011;20:36–44. - PubMed
-
- Wilmer A, Louie K, Dodek P, Wong H, Ayas N. Incidence of medication errors and adverse drug events in the ICU: a systematic review. Qual Saf Health Care. 2010;19:e7. Epub 2010 Jul 29. - PubMed
-
- Kane-Gill SL, Jacobi J, Rothschild JM. Adverse drug events in intensive care units: risk factors, impact, and the role of team care. Crit Care Med. 2010;38(Suppl.):S83–S9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
