

Interleukin 6, lipopolysaccharide-binding protein and interleukin 10 in the prediction of risk and etiologic patterns in patients with community-acquired pneumonia: results from the German competence network CAPNETZ
- PMID: 22348735
- PMCID: PMC3311562
- DOI: 10.1186/1471-2466-12-6
Interleukin 6, lipopolysaccharide-binding protein and interleukin 10 in the prediction of risk and etiologic patterns in patients with community-acquired pneumonia: results from the German competence network CAPNETZ
Abstract
Background: The aim of our study was to investigate the predictive value of the biomarkers interleukin 6 (IL-6), interleukin 10 (IL-10) and lipopolysaccharide-binding protein (LBP) compared with clinical CRB and CRB-65 severity scores in patients with community-acquired pneumonia (CAP).
Methods: Samples and data were obtained from patients enrolled into the German CAPNETZ study group. Samples (blood, sputum and urine) were collected within 24 h of first presentation and inclusion in the CAPNETZ study, and CRB and CRB-65 scores were determined for all patients at the time of enrollment. The combined end point representative of a severe course of CAP was defined as mechanical ventilation, intensive care unit treatment and/or death within 30 days. Overall, a total of 1,000 patients were enrolled in the study. A severe course of CAP was observed in 105 (10.5%) patients.
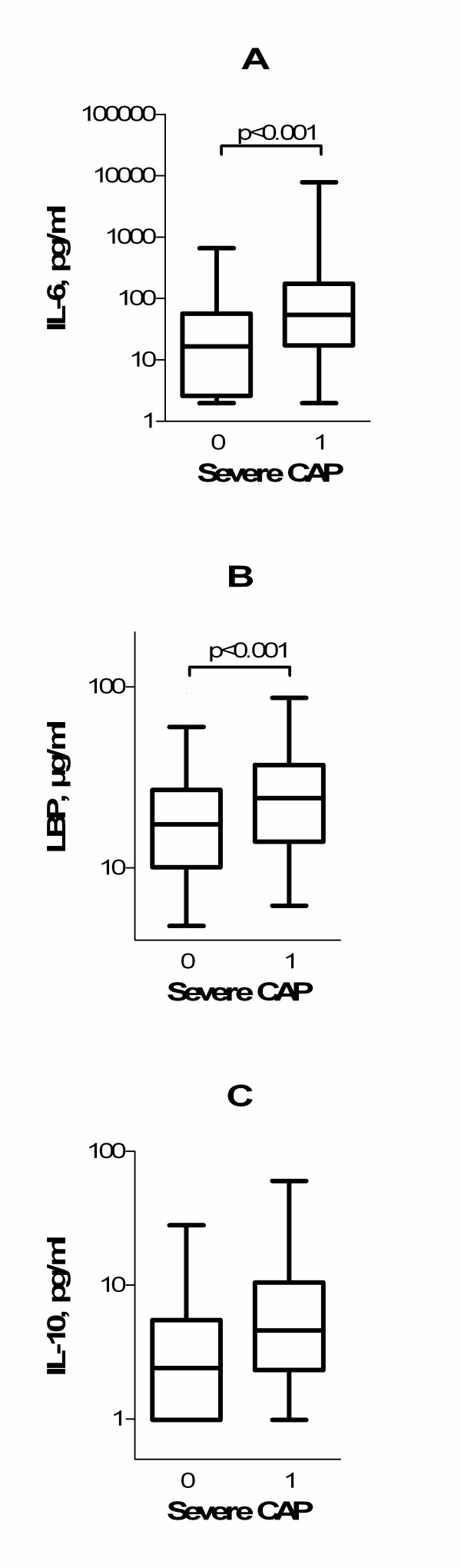
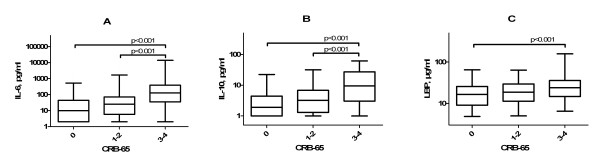
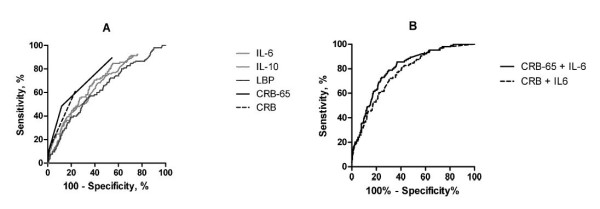
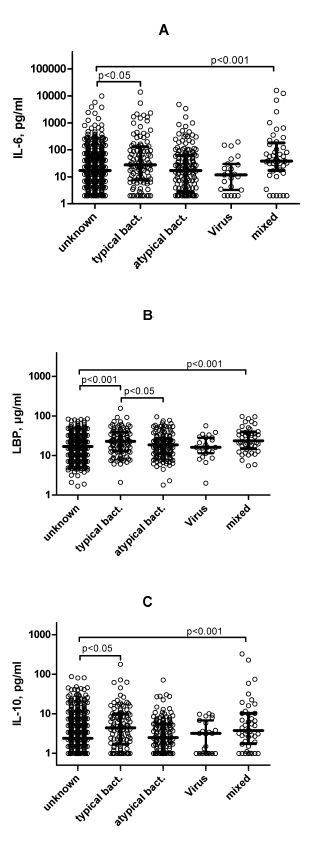
Results: The highest IL-6, IL-10 and LBP concentrations were found in patients with CRB-65 scores of 3-4 or CRB scores of 2-3. IL-6 and LBP levels on enrollment in the study were significantly higher for patients with a severe course of CAP than for those who did not have severe CAP. In receiver operating characteristic analyses, the area under the curve values for of IL-6 (0.689), IL-10 (0.665) and LPB (0.624) in a severe course of CAP were lower than that of CRB-65 (0.764) and similar to that of CRB (0.69). The accuracy of both CRB and CRB-65 was increased significantly by including IL-6 measurements. In addition, higher cytokine concentrations were found in patients with typical bacterial infections compared with patients with atypical or viral infections and those with infection of unknown etiology. LBP showed the highest discriminatory power with respect to the etiology of infection.
Conclusions: IL-6, IL-10 and LBP concentrations were increased in patients with a CRB-65 score of 3-4 and a severe course of CAP. The concentrations of IL-6 and IL-10 reflected the severity of disease in patients with CAP. The predictive power of IL-6, IL-10 and LBP for a severe course of pneumonia was lower than that of CRB-65. Typical bacterial pathogens induced the highest LBP, IL-6 and IL-10 concentrations.
© 2012 Zobel et al; licensee BioMed Central Ltd.
Figures
References
-
- Welte T, Suttorp N, Marre R. CAPNETZ-community-acquired pneumonia competence network. Infection. 2004;32:234–238. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
