

A practical guide to diagnostic transcranial magnetic stimulation: report of an IFCN committee
- PMID: 22349304
- PMCID: PMC4890546
- DOI: 10.1016/j.clinph.2012.01.010
A practical guide to diagnostic transcranial magnetic stimulation: report of an IFCN committee
Abstract
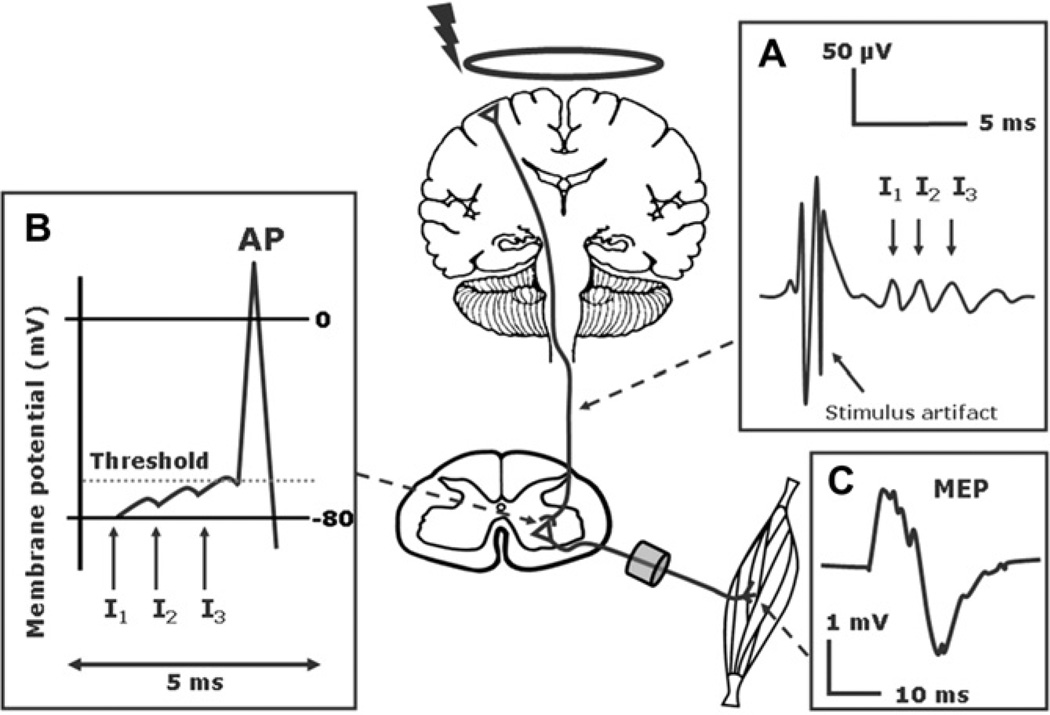
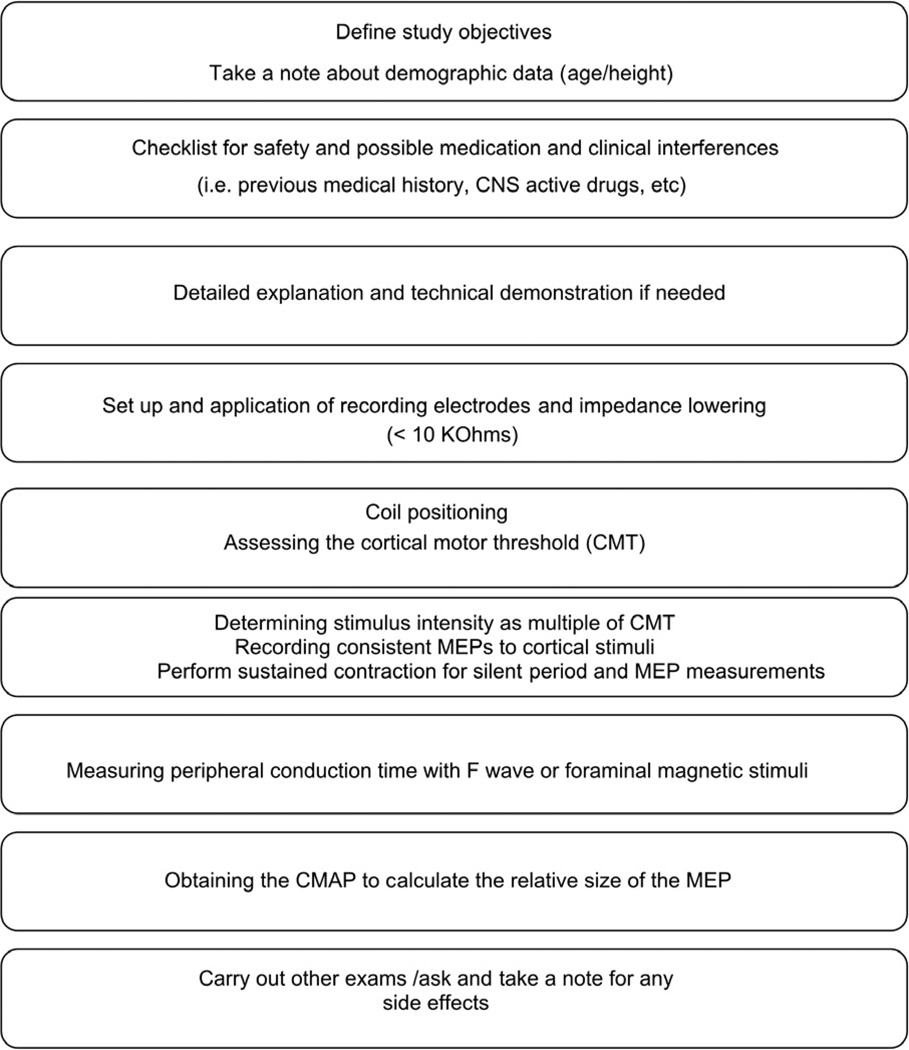
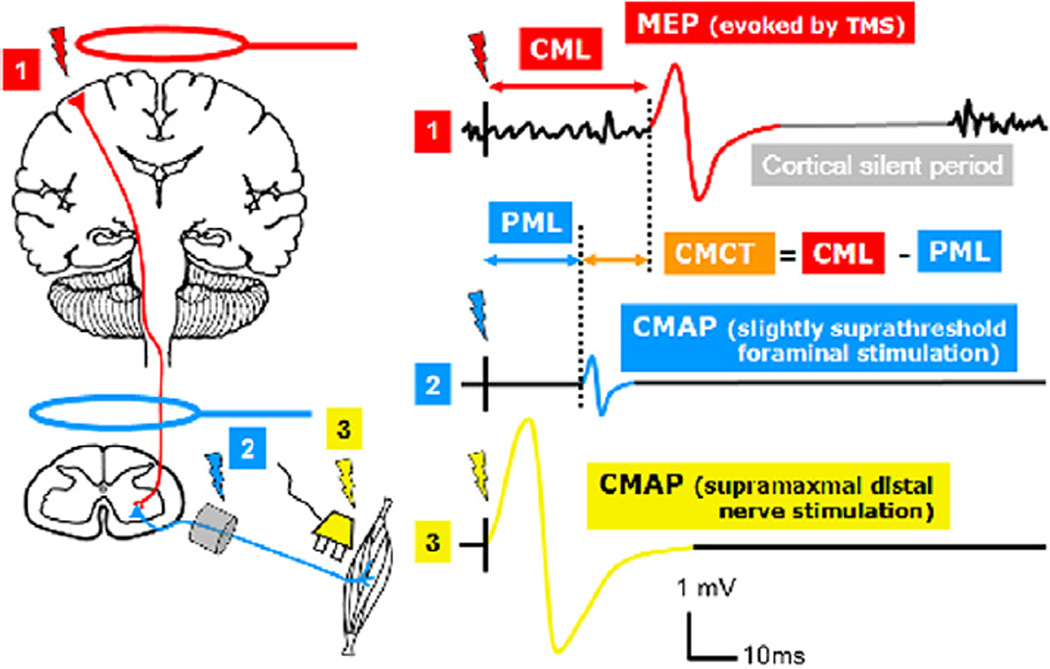
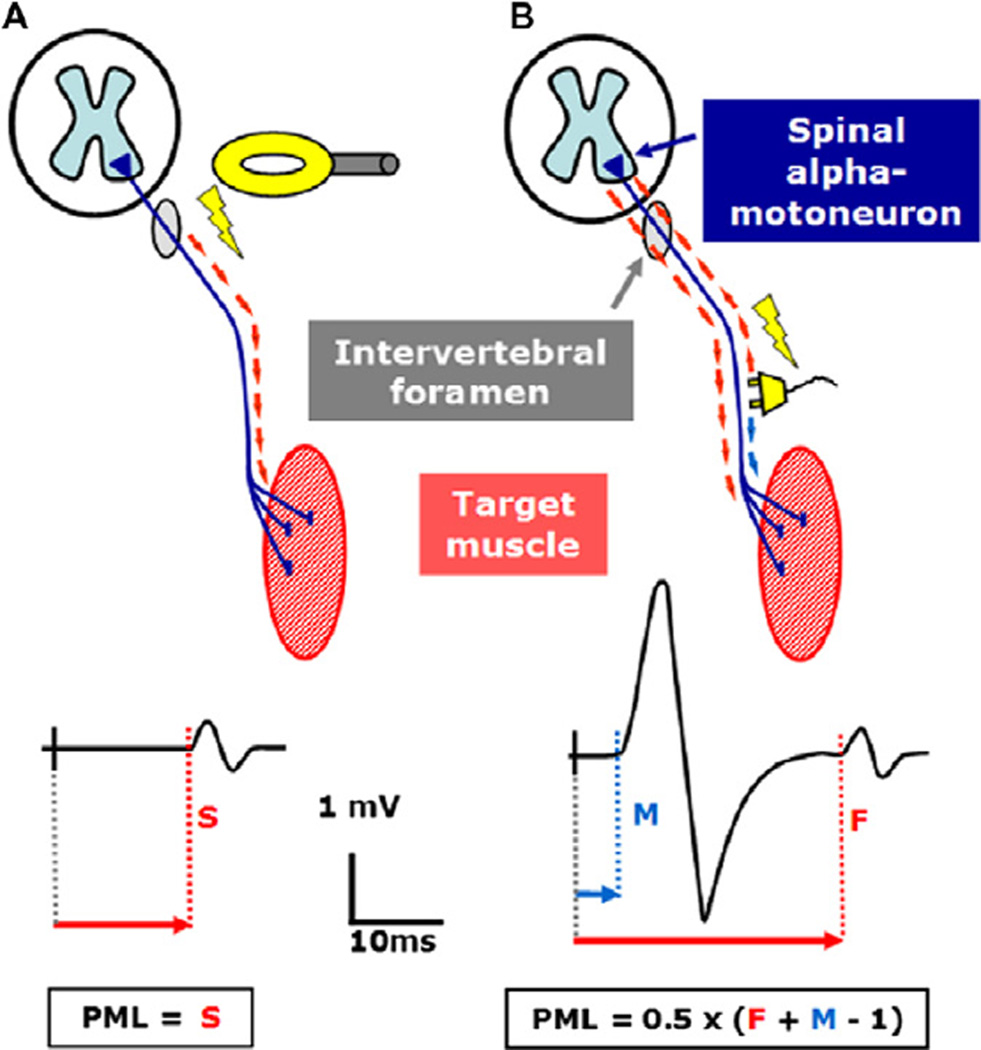
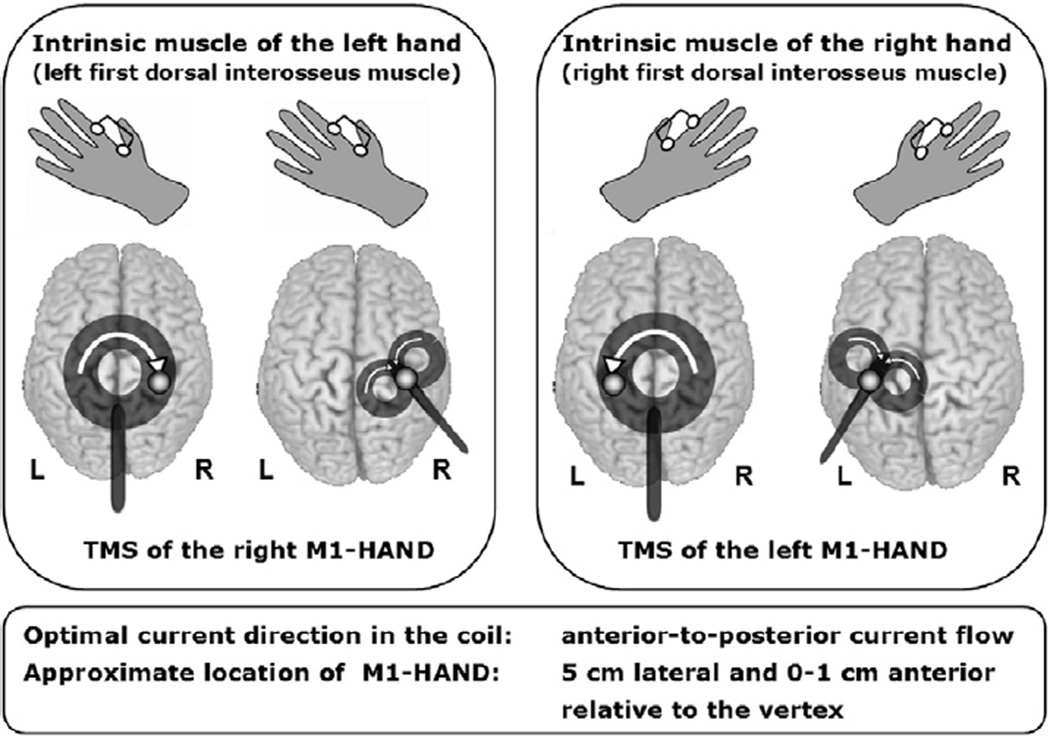
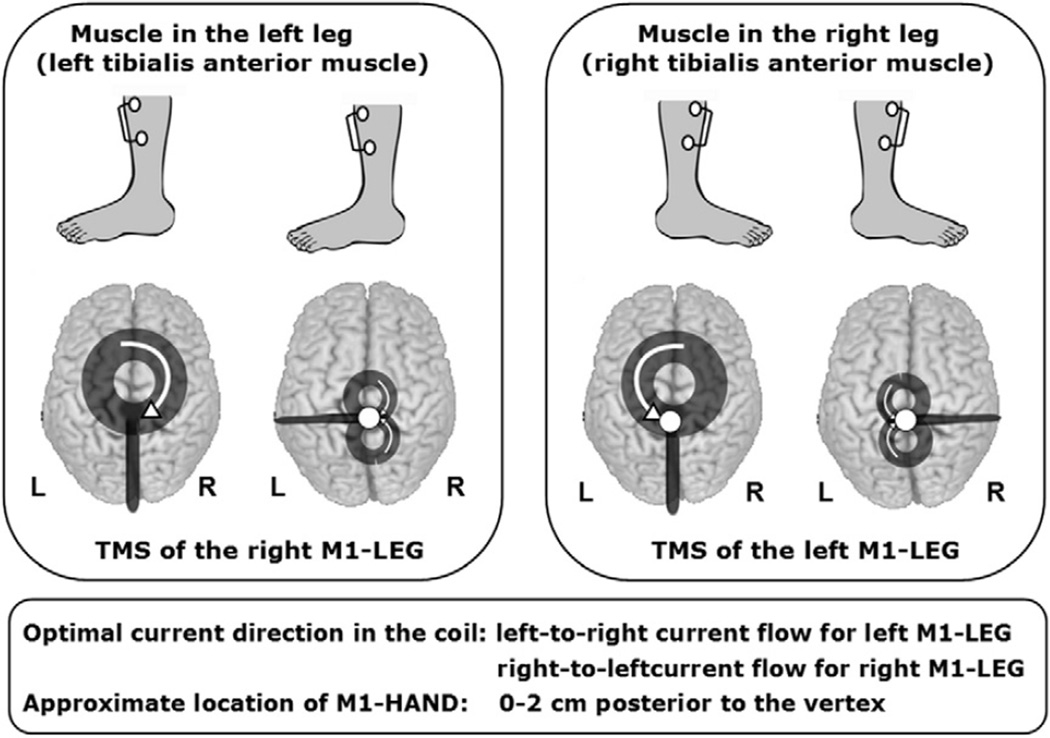
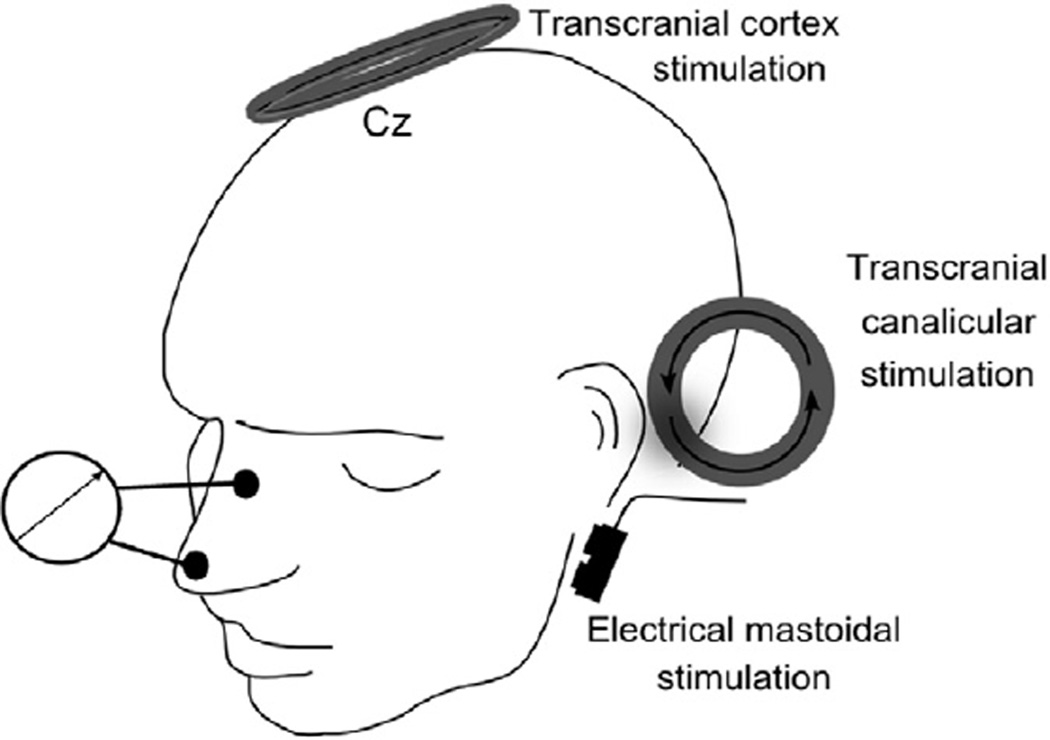
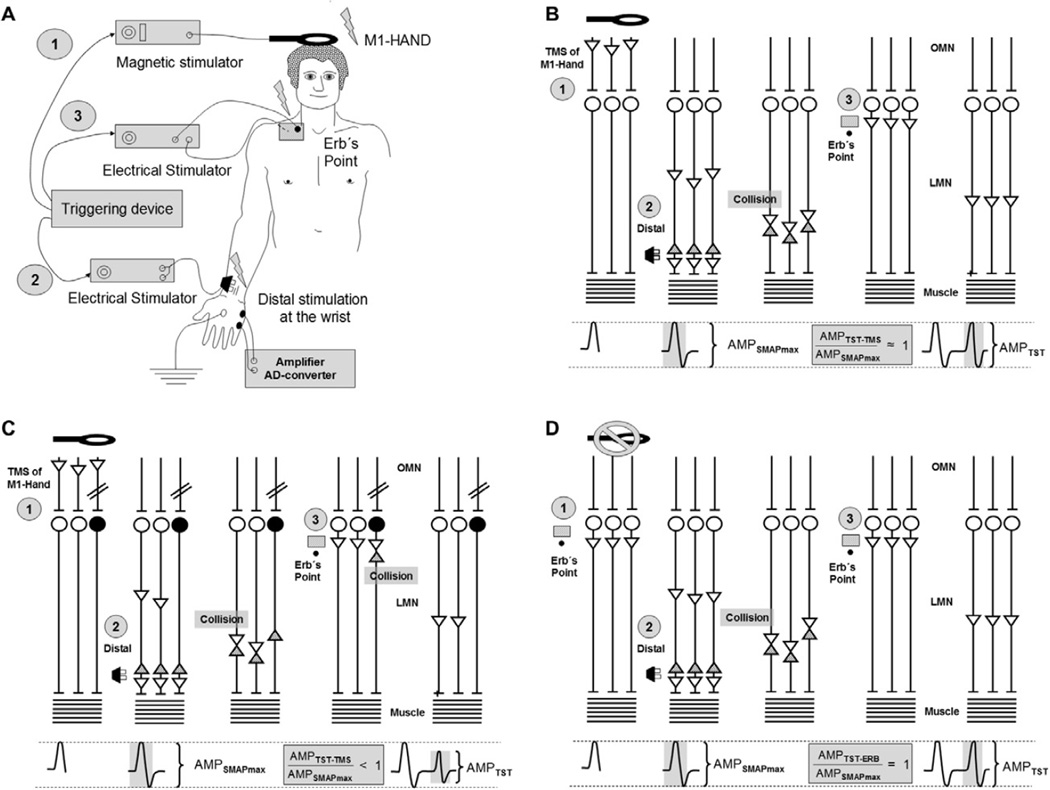
Transcranial magnetic stimulation (TMS) is an established neurophysiological tool to examine the integrity of the fast-conducting corticomotor pathways in a wide range of diseases associated with motor dysfunction. This includes but is not limited to patients with multiple sclerosis, amyotrophic lateral sclerosis, stroke, movement disorders, disorders affecting the spinal cord, facial and other cranial nerves. These guidelines cover practical aspects of TMS in a clinical setting. We first discuss the technical and physiological aspects of TMS that are relevant for the diagnostic use of TMS. We then lay out the general principles that apply to a standardized clinical examination of the fast-conducting corticomotor pathways with single-pulse TMS. This is followed by a detailed description of how to examine corticomotor conduction to the hand, leg, trunk and facial muscles in patients. Additional sections cover safety issues, the triple stimulation technique, and neuropediatric aspects of TMS.
Copyright © 2012 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
Figures
Comment in
-
On relative frequency estimation of transcranial magnetic stimulation motor threshold.Clin Neurophysiol. 2012 Nov;123(11):2319-20. doi: 10.1016/j.clinph.2012.04.014. Epub 2012 May 15. Clin Neurophysiol. 2012. PMID: 22591812 No abstract available.
References
-
- Amassian VE, Stewart M, Quirk GJ, Rosenthal JL. Physiological basis of motor effects of a transient stimulus to cerebral cortex. Neurosurgery. 1987;20:74–93. - PubMed
-
- Awiszus F. TMS and threshold hunting. Suppl Clin Neurophysiol. 2003;56:13–23. - PubMed
-
- Awiszus F. Fast estimation of transcranial magnetic stimulation motor threshold: is it safe? Brain Stimul. 2011;4:58–59. - PubMed
-
- Awiszus F, Feistner H. Kortikale Reizschwelle. Das TMS-Buch. 2007:149–158.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
