

Adult outcome of pediatric hydrocephalus
- PMID: 22349961
- PMCID: PMC3360844
- DOI: 10.1007/s00381-012-1723-y
Adult outcome of pediatric hydrocephalus
Abstract
Introduction: The outlook of pediatric hydrocephalus has spectacularly improved over the past decades; however, the adult outcome is still poorly documented. Determining the healthcare profile of these patients is important in order to organize the management of this growing population. We decided to review our pediatric hydrocephalus database for pediatric patients treated for hydrocephalus and followed up into adulthood.
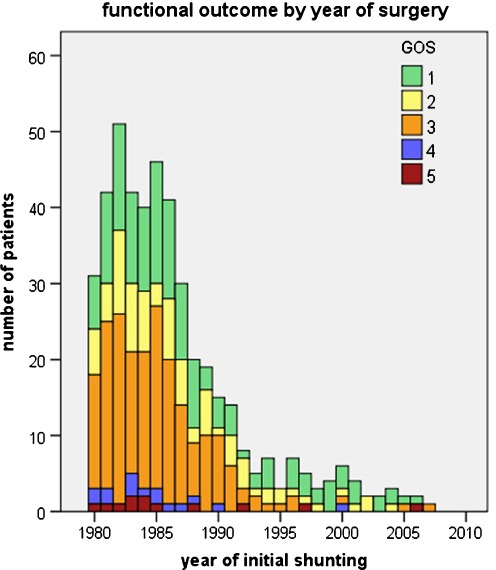
Methods: Our institution has a virtual monopoly for pediatric hydrocephalus, serving a four-million-plus population; the transition to adult care is also managed in the same institution. We retrospectively reviewed patients younger than 18 treated for hydrocephalus since 1980 and followed up beyond the age of 20.
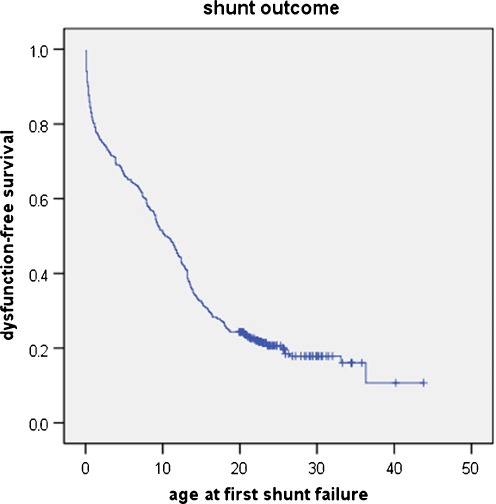
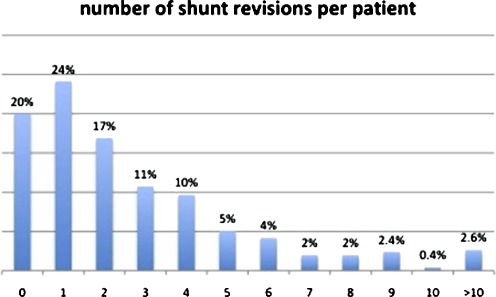
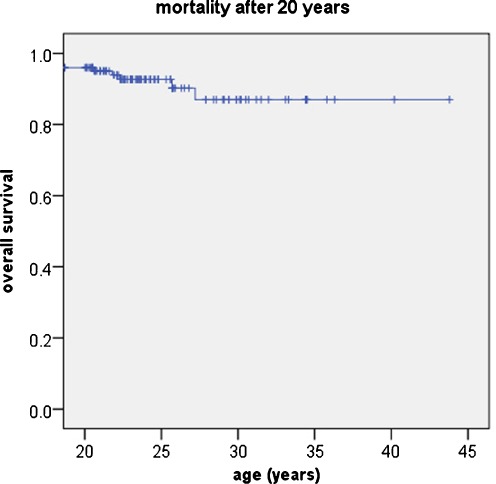
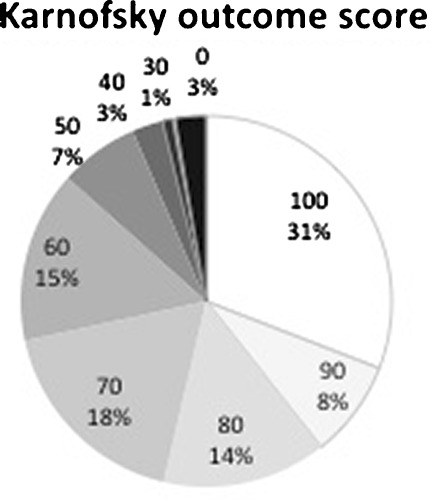
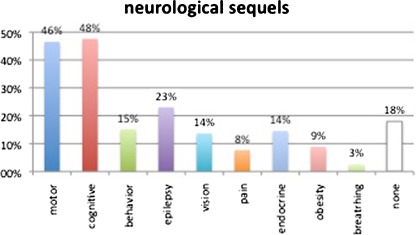
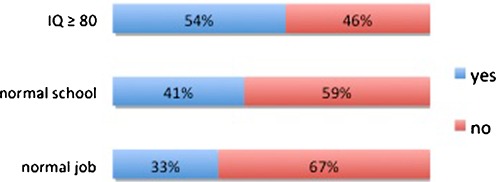
Results: We reviewed 456 patients, with a mean initial age of 55.6 months, and followed up for a mean of 24.2 years. In 81 patients (17.8%), the last shunt operation occurred after 20 years; 22 of these (4.9% of the total) having never been revised earlier. Sixteen patients (3.5%) could be weaned of their shunt. Thirteen patients died in adult age, 5 of these dying of shunt-related causes. The most prominent sequels were motor (46.5%) and cognitive (47.6%); only 82 patients (18.0%) had no sequel at all. Intelligence quotient values were ≥80 in 54.5% of tested patients; however, schooling was normal in only 41.4%, and only 33.7% was employed in the competitive labor market.
Conclusion: Adults treated for hydrocephalus in childhood require a life-long follow-up. Late mortality is low but not null, morbidity is high, and many patients require shunt surgery during adulthood. The transition from child to adult neurosurgery needs to be organized for these vulnerable patients.
Figures
References
-
- Cinalli G, Salazar C, Mallucci C, Yada JZ, Zerah M, Sainte-Rose C. The role of endoscopic third ventriculostomy in the management of shunt malfunction. Neurosurgery. 1998;43:1323–1327. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
