

Fetal and infant origins of asthma
- PMID: 22350146
- PMCID: PMC3292726
- DOI: 10.1007/s10654-012-9657-y
Fetal and infant origins of asthma
Abstract
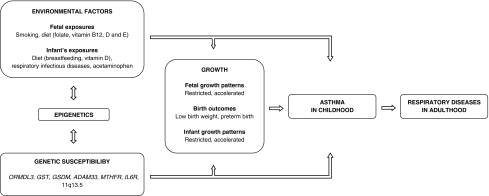
Previous studies have suggested that asthma, like other common diseases, has at least part of its origin early in life. Low birth weight has been shown to be associated with increased risks of asthma, chronic obstructive airway disease, and impaired lung function in adults, and increased risks of respiratory symptoms in early childhood. The developmental plasticity hypothesis suggests that the associations between low birth weight and diseases in later life are explained by adaptation mechanisms in fetal life and infancy in response to various adverse exposures. Various pathways leading from adverse fetal and infant exposures to growth adaptations and respiratory health outcomes have been studied, including fetal and early infant growth patterns, maternal smoking and diet, children's diet, respiratory tract infections and acetaminophen use, and genetic susceptibility. Still, the specific adverse exposures in fetal and early postnatal life leading to respiratory disease in adult life are not yet fully understood. Current studies suggest that both environmental and genetic factors in various periods of life, and their epigenetic mechanisms may underlie the complex associations of low birth weight with respiratory disease in later life. New well-designed epidemiological studies are needed to identify the specific underlying mechanisms. This review is focused on specific adverse fetal and infant growth patterns and exposures, genetic susceptibility, possible respiratory adaptations and perspectives for new studies.
Figures
References
-
- Asher MI, Montefort S, Bjorksten B, Lai CK, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC phases one and three repeat multicountry cross-sectional surveys. Lancet. 2006;368(9537):733–743. - PubMed
-
- Masoli M, Fabian D, Holt S, Beasley R. The global burden of asthma: executive summary of the GINA Dissemination Committee report. Allergy. 2004;59(5):469–478. - PubMed
-
- Peters SP, Jones CA, Haselkorn T, Mink DR, Valacer DJ, Weiss ST. Real-world evaluation of asthma control and treatment (REACT): findings from a national web-based survey. J Allergy Clin Immunol. 2007;119(6):1454–1461. - PubMed
-
- Behrens T. Current trends in aetiological asthma research. Eur J Epidemiol. 2009;24(3):115–118. - PubMed
-
- Reddel HK, Taylor DR, Bateman ED, Boulet LP, Boushey HA, Busse WW, et al. An official American Thoracic Society/European Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med. 2009;180(1):59–99. - PubMed
