

The risk-to-benefit ratio of transcatheter aortic valve implantation in specific patient cohorts: a single-centre experience
- PMID: 22350751
- PMCID: PMC3377897
- DOI: 10.1007/s00392-012-0426-4
The risk-to-benefit ratio of transcatheter aortic valve implantation in specific patient cohorts: a single-centre experience
Abstract
Background: Transcatheter aortic valve implantation (TAVI) has recently developed into an acceptable alternative to conventional surgery in high-risk patients. However, information on the identification of patients gaining most benefit from this procedure is still limited. The aim of this study was to evaluate safety and efficacy of TAVI in different patient cohorts.
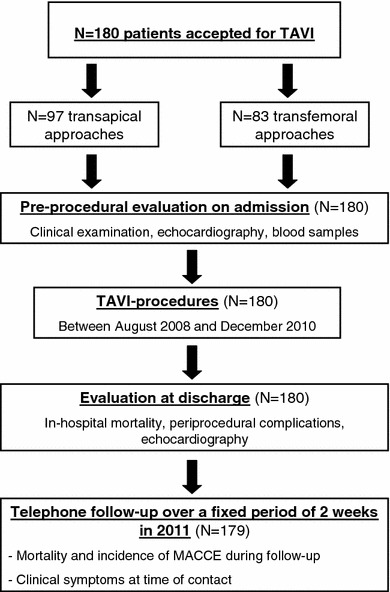
Methods: Between August 2008 and December 2010, 180 high-risk patients underwent TAVI at our institution (97 transapical and 83 transfemoral approaches). Periprocedural complications as well as mortality and incidence of MACCE during follow-up were recorded.
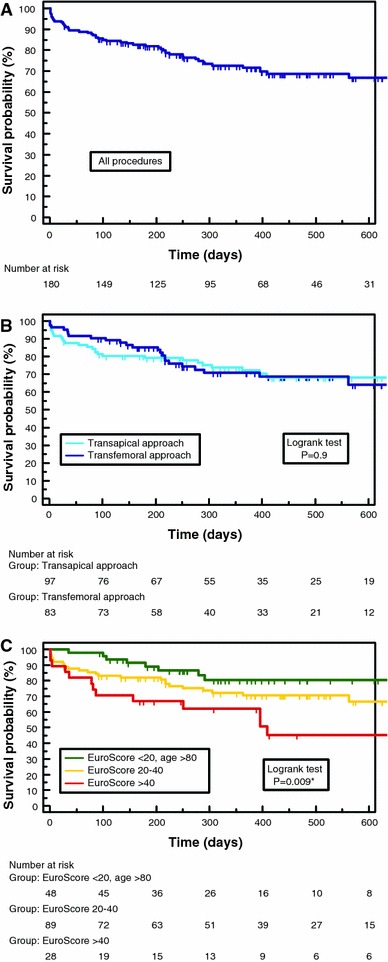
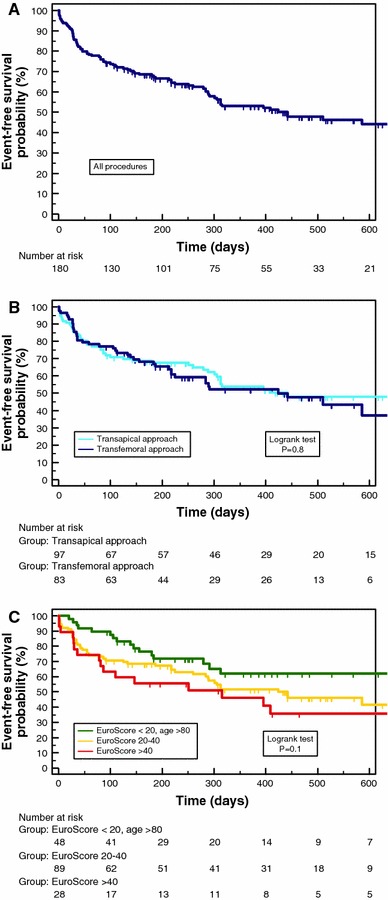
Results: Mean age was 82 ± 5 years, and mean logistic EuroScore 27 ± 14%. In the total cohort, 30-day mortality was 8.9% and 12-month survival (according to Kaplan-Meier-analysis) 72%, with no significant differences between the two approaches. However, a significant difference in survival was obvious after stratification of patients according to logistic EuroScore mortality estimates. Survival proportions at 1 year were 62% in patients with logistic EuroScore >40%, 71% in patients with EuroScore 20-40% and 80% in octogenarians with EuroScore <20% (P = 0.009). Furthermore, the observed median event-free survival as an indicator for morbidity ranged between 315 days in the first, 442 days in the second and 710 days in the third group (P = 0.1).
Conclusions: TAVI proved to be feasible with reproducible results. However, mortality and rehospitalization rates were considerably high in specific patient cohorts, suggesting that the risk-to-benefit ratio of TAVI should be validated individually. In the present study, octogenarians with logistic EuroScore <20% could be identified as candidates apparently gaining high benefit from the procedure.
Figures
References
-
- Vahanian A, Baumgartner H, Bax J, Butchart E, Dion R, Filippatos G, Flachskampf F, Hall R, Iung B, Kasprzak J, Nataf P, Tornos P, Torracca L, Wenink A. Guidelines on the management of valvular heart disease: the Task Force on the management of valvular heart disease of the European Society of Cardiology. Eur Heart J. 2007;28(2):230–268. doi: 10.1093/eurheartj/ehm354. - DOI - PubMed
-
- Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187–2198. doi: 10.1056/NEJMoa1103510. - DOI - PubMed
-
- Vahanian A, Alfieri O, Al-Attar N, Antunes M, Bax J, Cormier B, Cribier A, De JP, Fournial G, Kappetein AP, Kovac J, Ludgate S, Maisano F, Moat N, Mohr F, Nataf P, Pierard L, Pomar JL, Schofer J, Tornos P, Tuzcu M, van Hout B, Von Segesser LK, Walther T. Transcatheter valve implantation for patients with aortic stenosis: a position statement from the European Association of Cardio-Thoracic Surgery (EACTS) and the European Society of Cardiology (ESC), in collaboration with the European Association of Percutaneous Cardiovascular Interventions (EAPCI) Eur Heart J. 2008;29(11):1463–1470. doi: 10.1093/eurheartj/ehn183. - DOI - PubMed
-
- Figulla HR, Cremer J, Walther T, Gerckens U, Erbel R, Osterspey A, Zahn R. Positionspapier zur kathetergeführten Aortenklappenintervention. Kardiologe. 2009;1(3):199–206. doi: 10.1007/s12181-009-0183-4. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
