

Novel therapies for metastatic renal cell carcinoma: efforts to expand beyond the VEGF/mTOR signaling paradigm
- PMID: 22351744
- PMCID: PMC3297694
- DOI: 10.1158/1535-7163.MCT-11-0806
Novel therapies for metastatic renal cell carcinoma: efforts to expand beyond the VEGF/mTOR signaling paradigm
Abstract
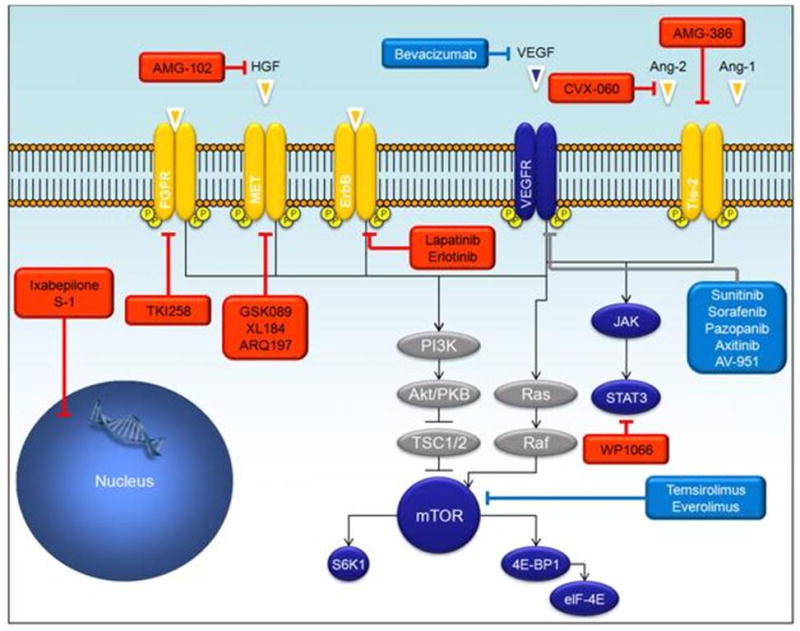
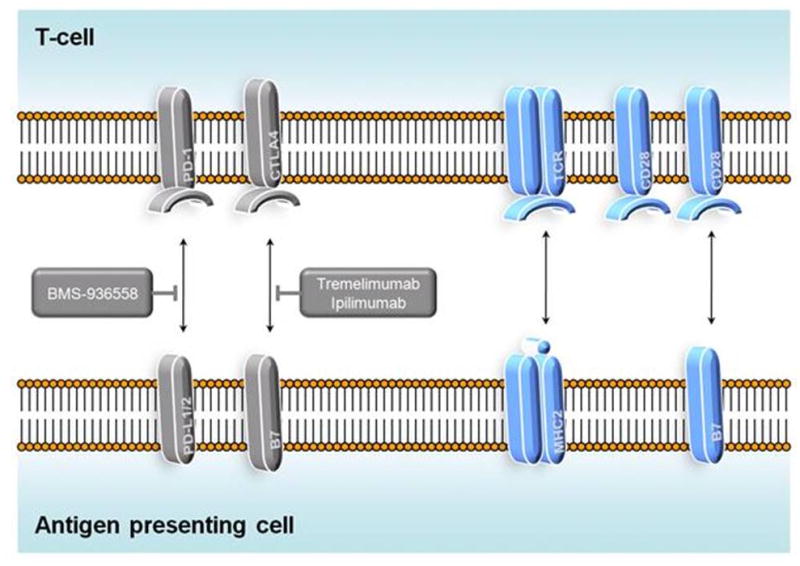
With six agents approved for metastatic renal cell carcinoma (mRCC) within the past 5 years, there has undoubtedly been progress in treating this disease. However, the goal of cure remains elusive, and the agents nearest approval (i.e., axitinib and tivozanib) abide by the same paradigm as existing drugs (i.e., inhibition of VEGF or mTOR signaling). The current review will focus on investigational agents that diverge from this paradigm. Specifically, novel immunotherapeutic strategies will be discussed, including vaccine therapy, cytotoxic T-lymphocyte antigen 4 (CTLA4) blockade, and programmed death-1 (PD-1) inhibition, as well as novel approaches to angiogenesis inhibition, such as abrogation of Ang/Tie-2 signaling. Pharmacologic strategies to block other potentially relevant signaling pathways, such as fibroblast growth factor receptor or MET inhibition, are also in various stages of development. Although VEGF and mTOR inhibition have dramatically improved outcomes for patients with mRCCs, a surge above the current plateau with these agents will likely require exploring new avenues.
Figures
References
-
- Fyfe G, Fisher RI, Rosenberg SA, Sznol M, Parkinson DR, Louie AC. Results of treatment of 255 patients with metastatic renal cell carcinoma who received high-dose recombinant interleukin-2 therapy. J Clin Oncol. 1995 Mar;13:688–96. - PubMed
-
- Motzer RJ, Bacik J, Murphy BA, Russo P, Mazumdar M. Interferon-Alfa as a Comparative Treatment for Clinical Trials of New Therapies Against Advanced Renal Cell Carcinoma. J Clin Oncol. 2002 January 1;20:289–96. - PubMed
-
- Hudes G, Carducci M, Tomczak P, Dutcher J, Figlin R, Kapoor A, et al. Temsirolimus, Interferon Alfa, or Both for Advanced Renal-Cell Carcinoma. N Engl J Med. 2007 May 31;356:2271–81. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
