

Silent cerebral infarcts: a review on a prevalent and progressive cause of neurologic injury in sickle cell anemia
- PMID: 22354000
- PMCID: PMC3367871
- DOI: 10.1182/blood-2011-02-272682
Silent cerebral infarcts: a review on a prevalent and progressive cause of neurologic injury in sickle cell anemia
Abstract
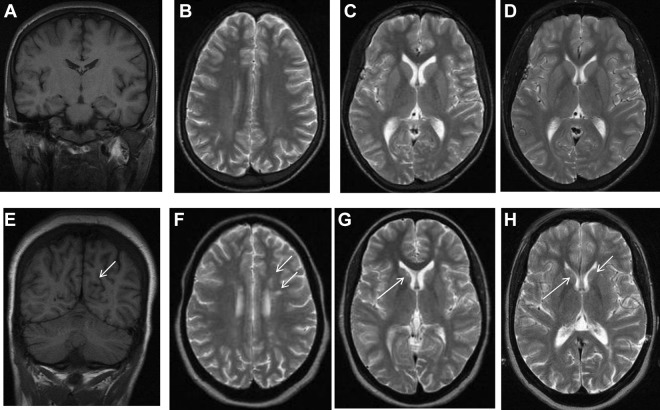
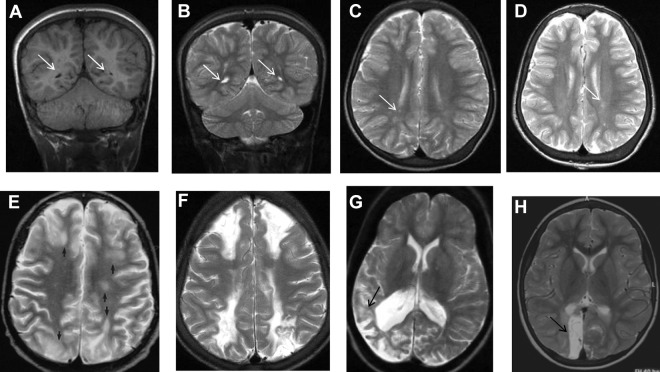
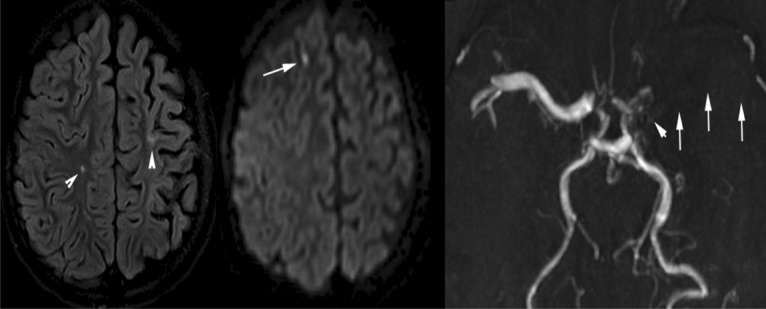
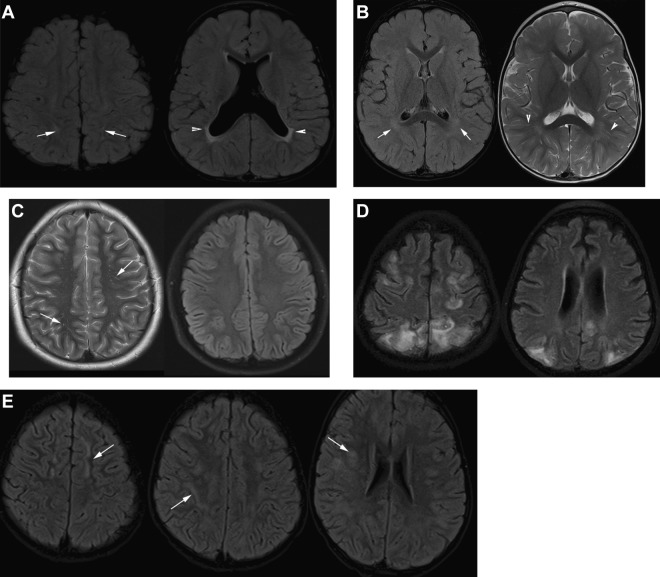
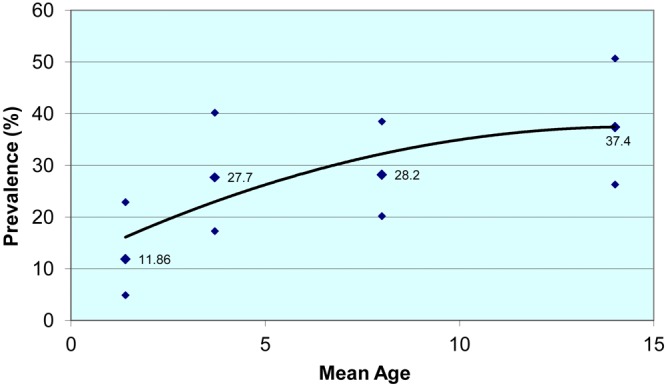
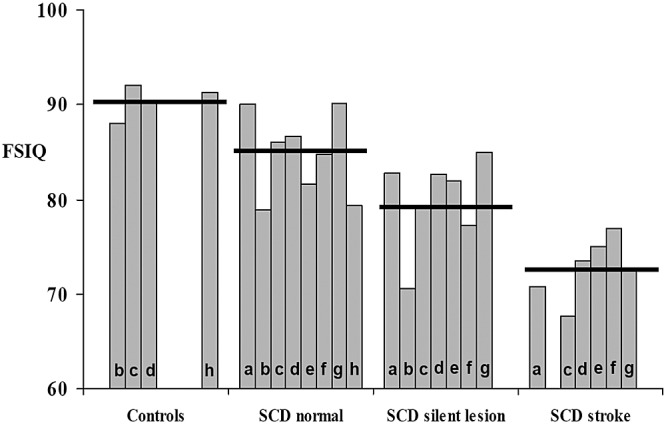
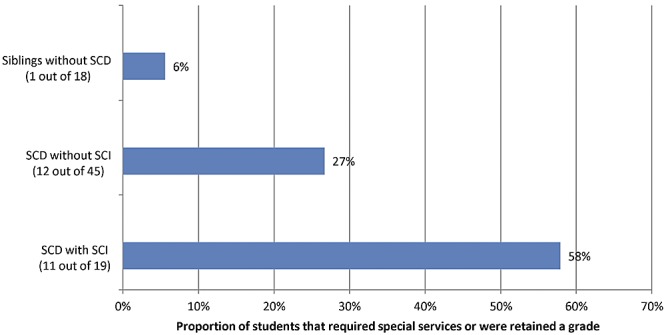
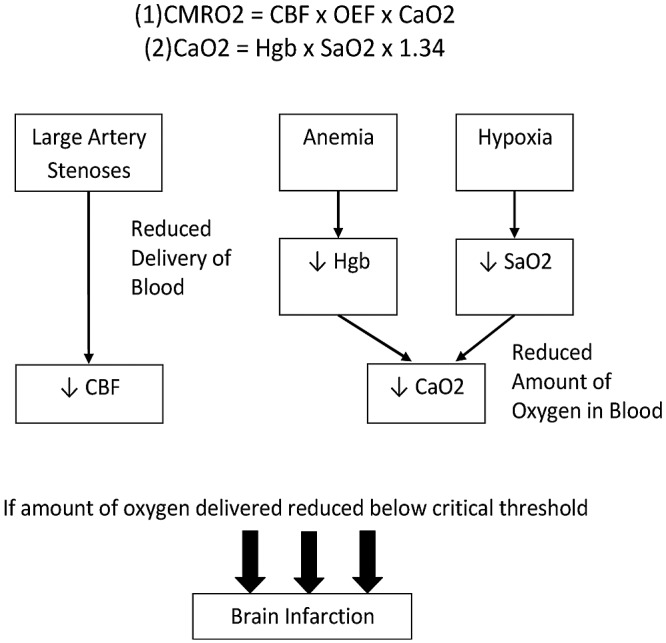
Silent cerebral infarct (SCI) is the most common form of neurologic disease in children with sickle cell anemia (SCA). SCI is defined as abnormal magnetic resonance imaging (MRI) of the brain in the setting of a normal neurologic examination without a history or physical findings associated with an overt stroke. SCI occurs in 27% of this population before their sixth, and 37% by their 14th birthdays. In adults with SCA, the clinical history of SCI is poorly defined, although recent evidence suggests that they too may have ongoing risk of progressive injury. Risk factors for SCI include male sex, lower baseline hemoglobin concentration, higher baseline systolic blood pressure, and previous seizures. Specific morbidity associated with SCI includes a decrement in general intellectual abilities, poor academic achievement, progression to overt stroke, and progressive SCI. In addition, children with previous stroke continue to have both overt strokes and new SCI despite receiving regular blood transfusion therapy for secondary stroke prevention. Studies that only include overt stroke as a measure of CNS injury significantly underestimate the total cerebral injury burden in this population. In this review, we describe the epidemiology, natural history, morbidity, medical management, and potential therapeutic options for SCI in SCA.
Figures
References
-
- Bernaudin F, Verlhac S, Arnaud C, et al. Impact of early transcranial Doppler screening and intensive therapy on cerebral vasculopathy outcome in a newborn sickle cell anemia cohort. Blood. 2011;117(4):1130–1140. quiz 1436. - PubMed
-
- Watkins KE, Hewes SKM, Connelly A, et al. Cognitive deficits associated with frontal-lobe infarction in children with sickle cell disease. Dev Med Child Neurol. 1998;40(8):536–543. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
