

Persistence of prolonged C-peptide production in type 1 diabetes as measured with an ultrasensitive C-peptide assay
- PMID: 22355018
- PMCID: PMC3322715
- DOI: 10.2337/dc11-1236
Persistence of prolonged C-peptide production in type 1 diabetes as measured with an ultrasensitive C-peptide assay
Abstract
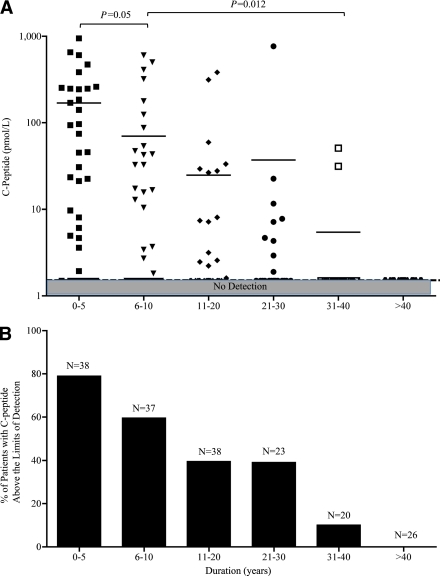
Objective: To examine persistence of C-peptide production by ultrasensitive assay years after onset of type 1 diabetes and factors associated with preserving β-cell function.
Research design and methods: Serum C-peptide levels, a marker of insulin production and surviving β-cells, were measured in human subjects (n = 182) by ultrasensitive assay, as was β-cell functioning. Twenty-two times more sensitive than standard assays, this assay's lower detection limit is 1.5 pmol/L. Disease duration, age at onset, age, sex, and autoantibody titers were analyzed by regression analysis to determine their relationship to C-peptide production. Another group of four patients was serially studied for up to 20 weeks to examine C-peptide levels and functioning.
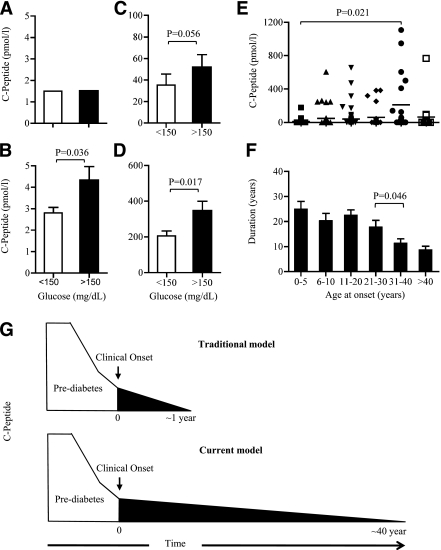
Results: The ultrasensitive assay detected C-peptide in 10% of individuals 31-40 years after disease onset and with percentages higher at shorter duration. Levels as low as 2.8 ± 1.1 pmol/L responded to hyperglycemia with increased C-peptide production, indicating residual β-cell functioning. Several other analyses showed that β-cells, whose C-peptide production was formerly undetectable, were capable of functioning. Multivariate analysis found disease duration (β = -2.721; P = 0.005) and level of zinc transporter 8 autoantibodies (β = 0.127; P = 0.015) significantly associated with C-peptide production. Unexpectedly, onset at >40 years of age was associated with low C-peptide production, despite short disease duration.
Conclusions: The ultrasensitive assay revealed that C-peptide production persists for decades after disease onset and remains functionally responsive. These findings suggest that patients with advanced disease, whose β-cell function was thought to have long ceased, may benefit from interventions to preserve β-cell function or to prevent complications.
Figures

Comment in
-
Dead or alive?Diabetes Care. 2012 Mar;35(3):459-60. doi: 10.2337/dc11-2441. Diabetes Care. 2012. PMID: 22355015 Free PMC article. No abstract available.
-
Diabetes: Functional β cells detected in long-standing T1DM--a new hope for intervention?Nat Rev Endocrinol. 2012 Mar 13;8(5):256. doi: 10.1038/nrendo.2012.32. Nat Rev Endocrinol. 2012. PMID: 22411432 No abstract available.
References
-
- Gianani R, Campbell-Thompson M, Sarkar SA, et al. Dimorphic histopathology of long-standing childhood-onset diabetes. Diabetologia 2010;53:690–698 - PubMed
-
- Madsbad S, Krarup T, Regeur L, Faber OK, Binder C. Insulin secretory reserve in insulin dependent patients at time of diagnosis and the first 180 days of insulin treatment. Acta Endocrinol (Copenh) 1980;95:359–363 - PubMed
-
- Steele C, Hagopian WA, Gitelman S, et al. Insulin secretion in type 1 diabetes. Diabetes 2004;53:426–433 - PubMed
-
- Eff Ch, Faber O, Deckert T. Persistent insulin secretion, assessed by plasma C-peptide estimation in long-term juvenile diabetics with a low insulin requirement. Diabetologia 1978;15:169–172 - PubMed
-
- Nakanishi K, Watanabe C. Rate of β-cell destruction in type 1 diabetes influences the development of diabetic retinopathy: protective effect of residual β-cell function for more than 10 years. J Clin Endocrinol Metab 2008;93:4759–4766 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
