

iTRAQ identification of candidate serum biomarkers associated with metastatic progression of human prostate cancer
- PMID: 22355332
- PMCID: PMC3280251
- DOI: 10.1371/journal.pone.0030885
iTRAQ identification of candidate serum biomarkers associated with metastatic progression of human prostate cancer
Abstract
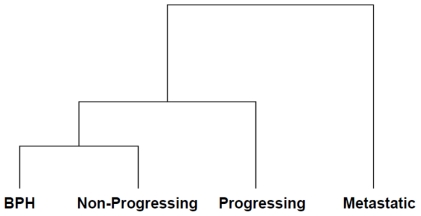
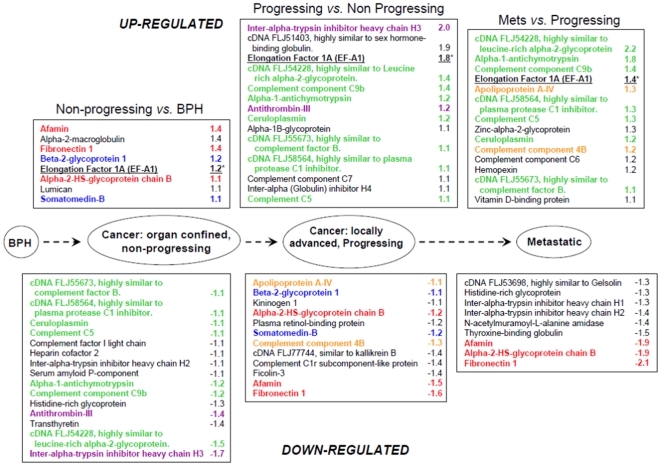
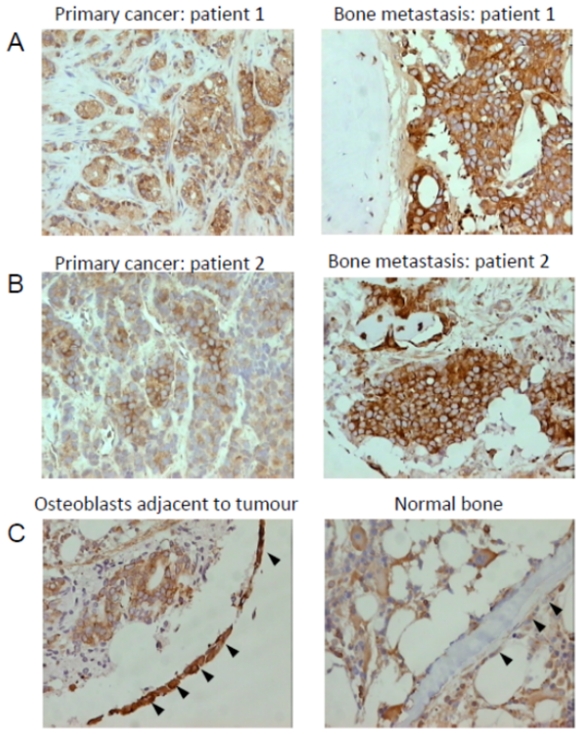
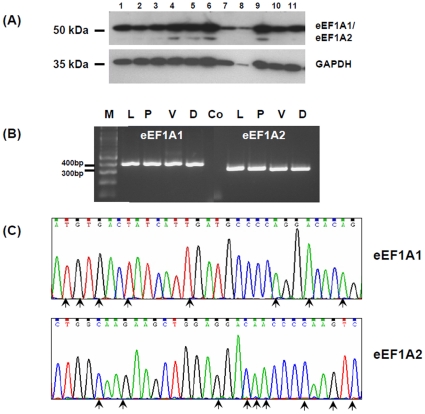
A major challenge in the management of patients with prostate cancer is identifying those individuals at risk of developing metastatic disease, as in most cases the disease will remain indolent. We analyzed pooled serum samples from 4 groups of patients (n = 5 samples/group), collected prospectively and actively monitored for a minimum of 5 yrs. Patients groups were (i) histological diagnosis of benign prostatic hyperplasia with no evidence of cancer 'BPH', (ii) localised cancer with no evidence of progression, 'non-progressing' (iii) localised cancer with evidence of biochemical progression, 'progressing', and (iv) bone metastasis at presentation 'metastatic'. Pooled samples were immuno-depleted of the 14 most highly abundant proteins and analysed using a 4-plex iTRAQ approach. Overall 122 proteins were identified and relatively quantified. Comparisons of progressing versus non-progressing groups identified the significant differential expression of 25 proteins (p<0.001). Comparisons of metastatic versus progressing groups identified the significant differential expression of 23 proteins. Mapping the differentially expressed proteins onto the prostate cancer progression pathway revealed the dysregulated expression of individual proteins, pairs of proteins and 'panels' of proteins to be associated with particular stages of disease development and progression. The median immunostaining intensity of eukaryotic translation elongation factor 1 alpha 1 (eEF1A1), one of the candidates identified, was significantly higher in osteoblasts in close proximity to metastatic tumour cells compared with osteoblasts in control bone (p = 0.0353, Mann Whitney U). Our proteomic approach has identified leads for potentially useful serum biomarkers associated with the metastatic progression of prostate cancer. The panels identified, including eEF1A1 warrant further investigation and validation.
Conflict of interest statement
Figures
References
-
- Damber JE, Aus G. Prostate cancer. Lancet. 2008;371:1710–1721. - PubMed
-
- Gronberg H. Prostate cancer epidemiology. Lancet. 2003;361:859–864. - PubMed
-
- Freedland SJ, Humphreys EB, Mangold LA, Eisenberger M, Dorey FJ, et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA. 2005;294:433–439. - PubMed
-
- Zhu X, van Leeuwen PJ, Bul M, Bangma CH, Roobol MJ, et al. Identifying and characterizing “escapes”- men who develop metastases or die from prostate cancer despite screening (ERSPC, section Rotterdam). Int J Cancer. 2011;129:2847–2854. - PubMed
-
- LaSpina M, Haas GP. Update on the diagnosis and management of prostate cancer. Can J Urol. 2008;15(Suppl 1):3–13; discussion 13. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
