

Impaired crossed facilitation of the corticospinal pathway after cervical spinal cord injury
- PMID: 22357796
- PMCID: PMC3774586
- DOI: 10.1152/jn.00850.2011
Impaired crossed facilitation of the corticospinal pathway after cervical spinal cord injury
Abstract
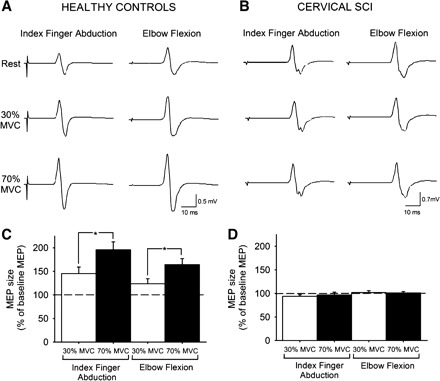
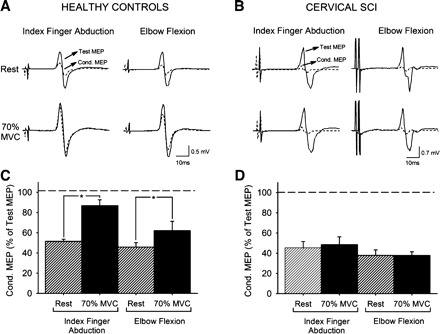
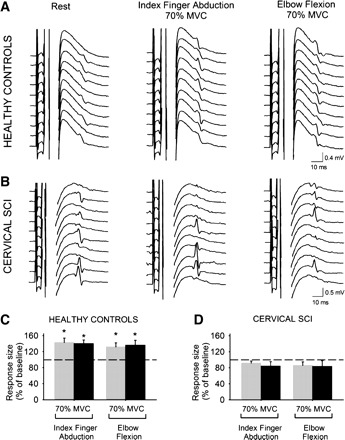
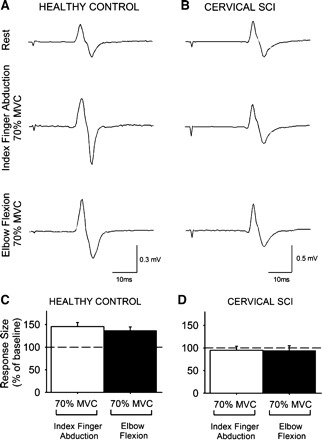
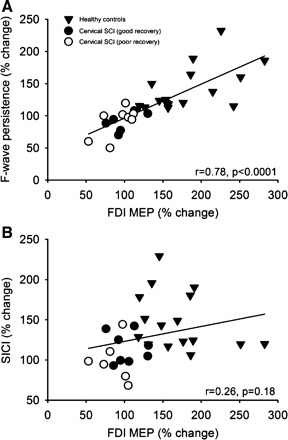
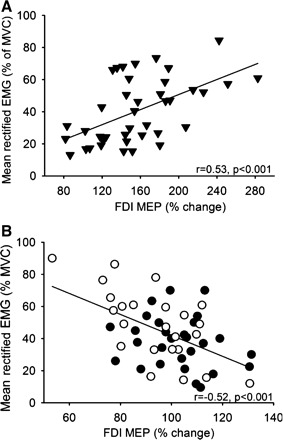
In uninjured humans, it is well established that voluntary contraction of muscles on one side of the body can facilitate transmission in the contralateral corticospinal pathway. This crossed facilitatory effect may favor interlimb coordination and motor performance. Whether this aspect of corticospinal function is preserved after chronic spinal cord injury (SCI) is unknown. Here, using transcranial magnetic stimulation, we show in patients with chronic cervical SCI (C(5)-C(8)) that the size of motor evoked potentials (MEPs) in a resting intrinsic hand muscle remained unchanged during increasing levels of voluntary contraction with a contralateral distal or proximal arm muscle. In contrast, MEP size in a resting hand muscle was increased during the same motor tasks in healthy control subjects. The magnitude of voluntary electromyography was negatively correlated with MEP size after chronic cervical SCI and positively correlated in healthy control subjects. To examine the mechanisms contributing to MEP crossed facilitation we examined short-interval intracortical inhibition (SICI), interhemispheric inhibition (IHI), and motoneuronal behavior by testing F waves and cervicomedullary MEPs (CMEPs). During strong voluntary contractions SICI was unchanged after cervical SCI and decreased in healthy control subjects compared with rest. F-wave amplitude and persistence and CMEP size remained unchanged after cervical SCI and increased in healthy control subjects compared with rest. In addition, during strong voluntary contractions IHI was unchanged in cervical SCI compared with rest. Our results indicate that GABAergic intracortical circuits, interhemispheric glutamatergic projections between motor cortices, and excitability of index finger motoneurons are neural mechanisms underlying, at least in part, the lack of crossed corticospinal facilitation observed after SCI. Our data point to the spinal motoneurons as a critical site for modulating corticospinal transmission after chronic cervical SCI.
Figures
References
-
- Barthélemy D, Willerslev-Olsen M, Lundell H, Conway BA, Knudsen H, Biering-Sørensen F, Nielsen JB. Impaired transmission in the corticospinal tract and gait disability in spinal cord injured persons. J Neurophysiol 104: 1167–1176, 2010 - PubMed
-
- Bennett DJ, Sanelli L, Cooke CL, Harvey PJ, Gorassini MA. Spastic long-lasting reflexes in the awake rat after sacral spinal cord injury. J Neurophysiol 91: 2247–2258, 2004 - PubMed
-
- Butler JE, Thomas CK. Effects of sustained stimulation on the excitability of motoneurons innervating paralyzed and control muscles. J Appl Physiol 94: 567–575, 2003 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical