

Cost-effectiveness of adult vaccination strategies using pneumococcal conjugate vaccine compared with pneumococcal polysaccharide vaccine
- PMID: 22357831
- PMCID: PMC3924773
- DOI: 10.1001/jama.2012.169
Cost-effectiveness of adult vaccination strategies using pneumococcal conjugate vaccine compared with pneumococcal polysaccharide vaccine
Abstract
Context: The cost-effectiveness of 13-valent pneumococcal conjugate vaccine (PCV13) compared with 23-valent pneumococcal polysaccharide vaccine (PPSV23) among US adults is unclear.
Objective: To estimate the cost-effectiveness of PCV13 vaccination strategies in adults.
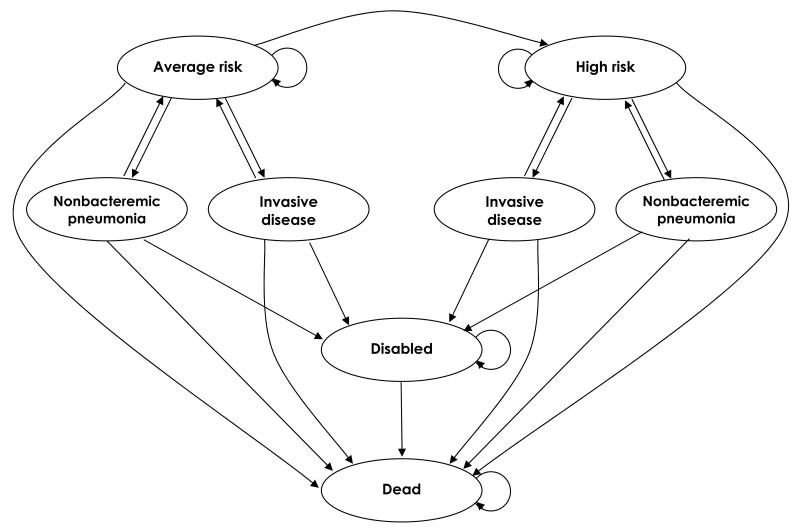
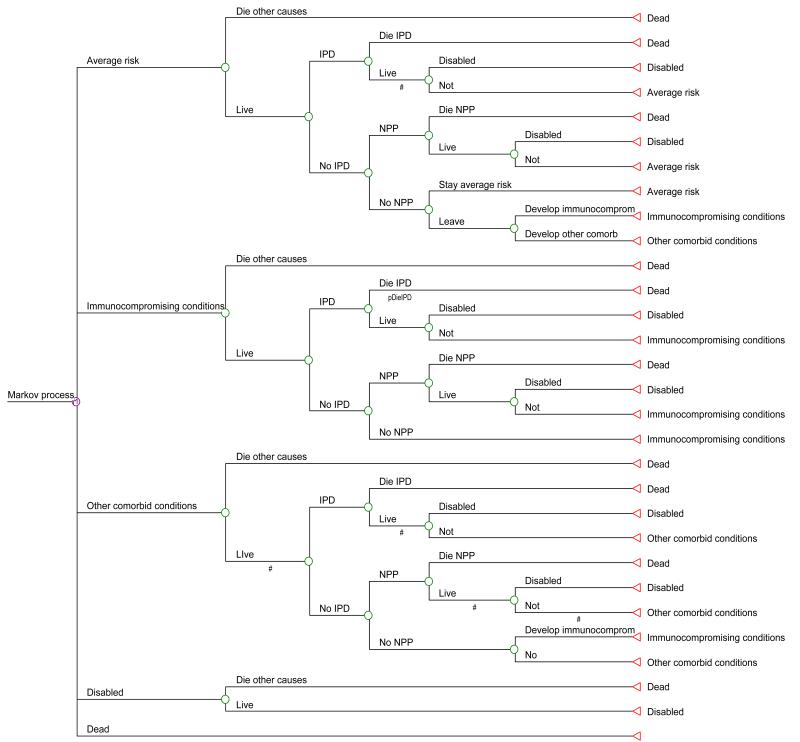
Design, setting, and participants: A Markov state-transition model, lifetime time horizon, societal perspective. Simulations were performed in hypothetical cohorts of US 50-year-olds. Vaccination strategies and effectiveness estimates were developed by a Delphi expert panel; indirect (herd immunity) effects resulting from childhood PCV13 vaccination were extrapolated based on observed PCV7 effects. Data sources for model parameters included Centers for Disease Control and Prevention Active Bacterial Core surveillance, National Hospital Discharge Survey and Nationwide Inpatient Sample data, and the National Health Interview Survey.
Main outcome measures: Pneumococcal disease cases prevented and incremental costs per quality-adjusted life-year (QALY) gained.
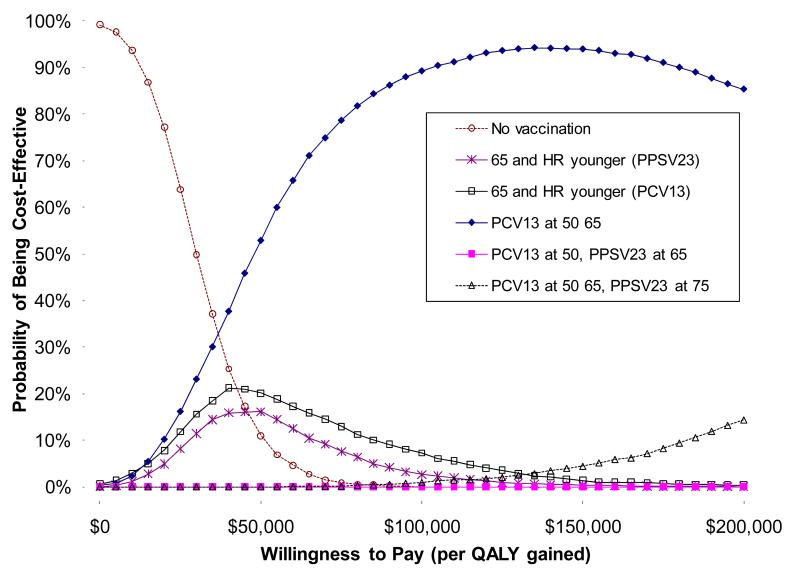
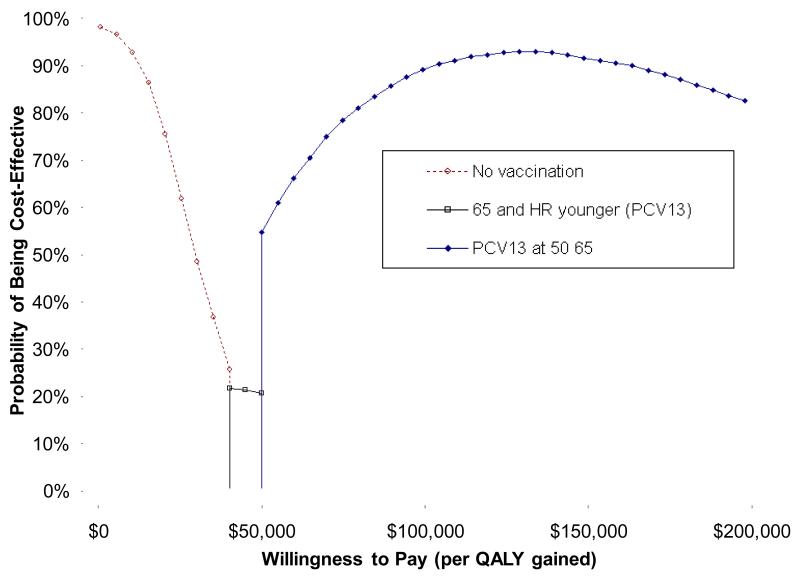
Results: In the base case scenario, administration of PCV13 as a substitute for PPSV23 in current recommendations (ie, vaccination at age 65 years and at younger ages if comorbidities are present) cost $28,900 per QALY gained compared with no vaccination and was more cost-effective than the currently recommended PPSV23 strategy. Routine PCV13 at ages 50 and 65 years cost $45,100 per QALY compared with PCV13 substituted in current recommendations. Adding PPSV23 at age 75 years to PCV13 at ages 50 and 65 years gained 0.00002 QALYs, costing $496,000 per QALY gained. Results were robust in sensitivity analyses and alternative scenarios, except when low PCV13 effectiveness against nonbacteremic pneumococcal pneumonia was assumed or when greater childhood vaccination indirect effects were modeled. In these cases, PPSV23 as currently recommended was favored.
Conclusion: Overall, PCV13 vaccination was favored compared with PPSV23, but the analysis was sensitive to assumptions about PCV13 effectiveness against nonbacteremic pneumococcal pneumonia and the magnitude of potential indirect effects from childhood PCV13 on pneumococcal serotype distribution.
Figures
Comment in
-
Prevention of pneumococcal infection with vaccines: an evolving story.JAMA. 2012 Feb 22;307(8):847-9. doi: 10.1001/jama.2012.194. JAMA. 2012. PMID: 22357836 No abstract available.
Similar articles
-
Cost-effectiveness analysis of 13-valent pneumococcal conjugate vaccine versus 23-valent pneumococcal polysaccharide vaccine in an adult population in South Korea.Hum Vaccin Immunother. 2018;14(8):1914-1922. doi: 10.1080/21645515.2018.1456602. Epub 2018 Jul 11. Hum Vaccin Immunother. 2018. PMID: 29953307 Free PMC article.
-
Cost-effectiveness of pneumococcal vaccination strategies for the elderly in Korea.PLoS One. 2017 May 12;12(5):e0177342. doi: 10.1371/journal.pone.0177342. eCollection 2017. PLoS One. 2017. PMID: 28498857 Free PMC article.
-
Cost-effectiveness of the 13-valent pneumococcal conjugate vaccine in adults in Portugal versus "no vaccination" and versus vaccination with the 23-valent pneumococcal polysaccharide vaccine.Hum Vaccin Immunother. 2019;15(4):850-858. doi: 10.1080/21645515.2018.1560769. Epub 2019 Feb 20. Hum Vaccin Immunother. 2019. PMID: 30633615 Free PMC article.
-
Systematic literature review of cost-effectiveness analyses of adult 15- and 20-valent pneumococcal vaccines.Vaccine. 2025 Feb 6;46:126656. doi: 10.1016/j.vaccine.2024.126656. Epub 2024 Dec 27. Vaccine. 2025. PMID: 39731806
-
Cost-Effectiveness of Pneumococcal Vaccines for Adults Aged 65 Years and Older in Argentina.Value Health Reg Issues. 2022 Mar;28:76-81. doi: 10.1016/j.vhri.2021.08.003. Epub 2021 Nov 18. Value Health Reg Issues. 2022. PMID: 34801962
Cited by
-
Respiratory review of 2012: pneumonia.Tuberc Respir Dis (Seoul). 2012 Aug;73(2):77-83. doi: 10.4046/trd.2012.73.2.77. Epub 2012 Aug 31. Tuberc Respir Dis (Seoul). 2012. PMID: 23166539 Free PMC article.
-
Cost-effectiveness analysis of 13-valent pneumococcal conjugate vaccine versus 23-valent pneumococcal polysaccharide vaccine in an adult population in South Korea.Hum Vaccin Immunother. 2018;14(8):1914-1922. doi: 10.1080/21645515.2018.1456602. Epub 2018 Jul 11. Hum Vaccin Immunother. 2018. PMID: 29953307 Free PMC article.
-
Should UK Pneumococcal Vaccine Eligibility Criteria Include Alcohol Dependency in Areas with High Alcohol-Related Mortality?Vaccines (Basel). 2018 May 2;6(2):25. doi: 10.3390/vaccines6020025. Vaccines (Basel). 2018. PMID: 29724023 Free PMC article.
-
Cost-effectiveness of new adult pneumococcal vaccination strategies in Italy.Hum Vaccin Immunother. 2013 Mar;9(3):699-706. doi: 10.4161/hv.23268. Epub 2013 Jan 7. Hum Vaccin Immunother. 2013. PMID: 23295824 Free PMC article.
-
Herd immunity in older adults from a middle-income country: A time-series trend analysis of community-acquired pneumonia mortality 2003-2017.Health Sci Rep. 2023 May 3;6(5):e1224. doi: 10.1002/hsr2.1224. eCollection 2023 May. Health Sci Rep. 2023. PMID: 37152218 Free PMC article.
References
-
- Centers for Disease Control and Prevention Updated recommendations for prevention of invasive pneumococcal disease among adults using the 23-valent pneumococcal polysaccharide vaccine (PPSV23) MMWR Morb Mortal Wkly Rep. 2010;59(34):1102–6. - PubMed
-
- Metersky ML, Dransfield MT, Jackson LA. Determining the optimal pneumococcal vaccination strategy for adults: is there a role for the pneumococcal conjugate vaccine? Chest. 2010;138(3):486–90. - PubMed
-
- Moberley SA, Holden J, Tatham DP, Andrews RM. Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst Rev. 2008;(1):CD000422. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
