

Patterns of failure after treatment of atypical meningioma with gamma knife radiosurgery
- PMID: 22359231
- PMCID: PMC3794718
- DOI: 10.1007/s11060-012-0828-1
Patterns of failure after treatment of atypical meningioma with gamma knife radiosurgery
Abstract
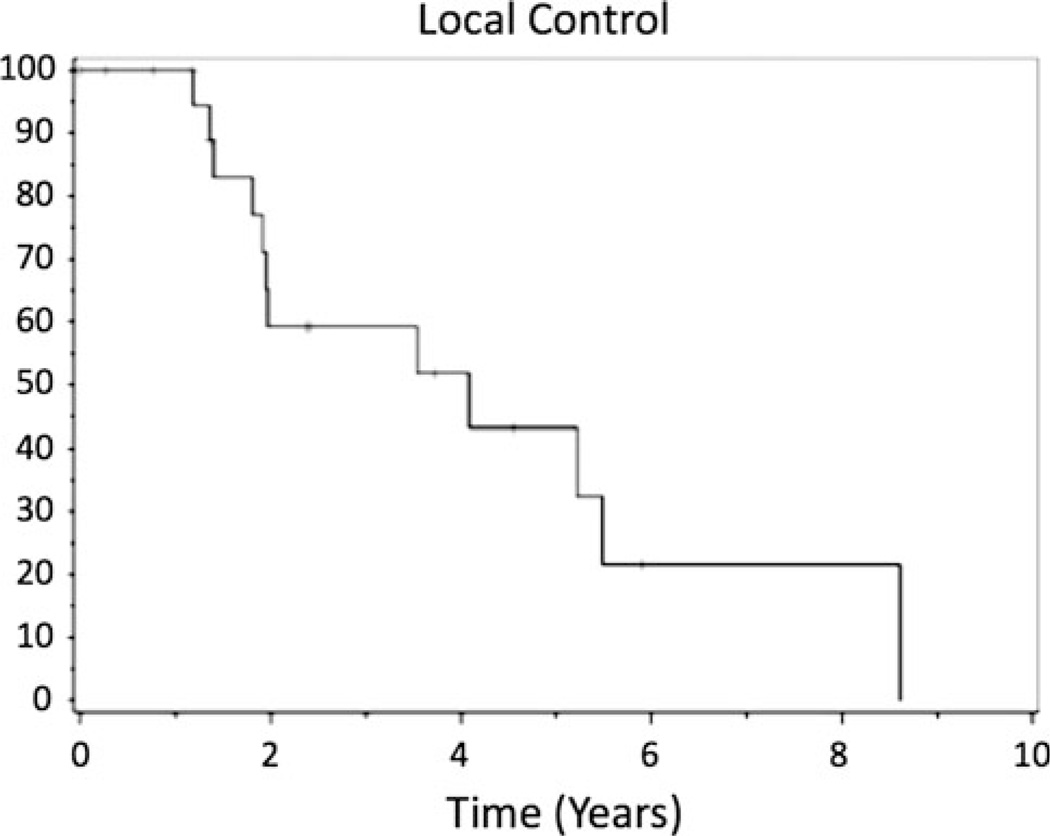
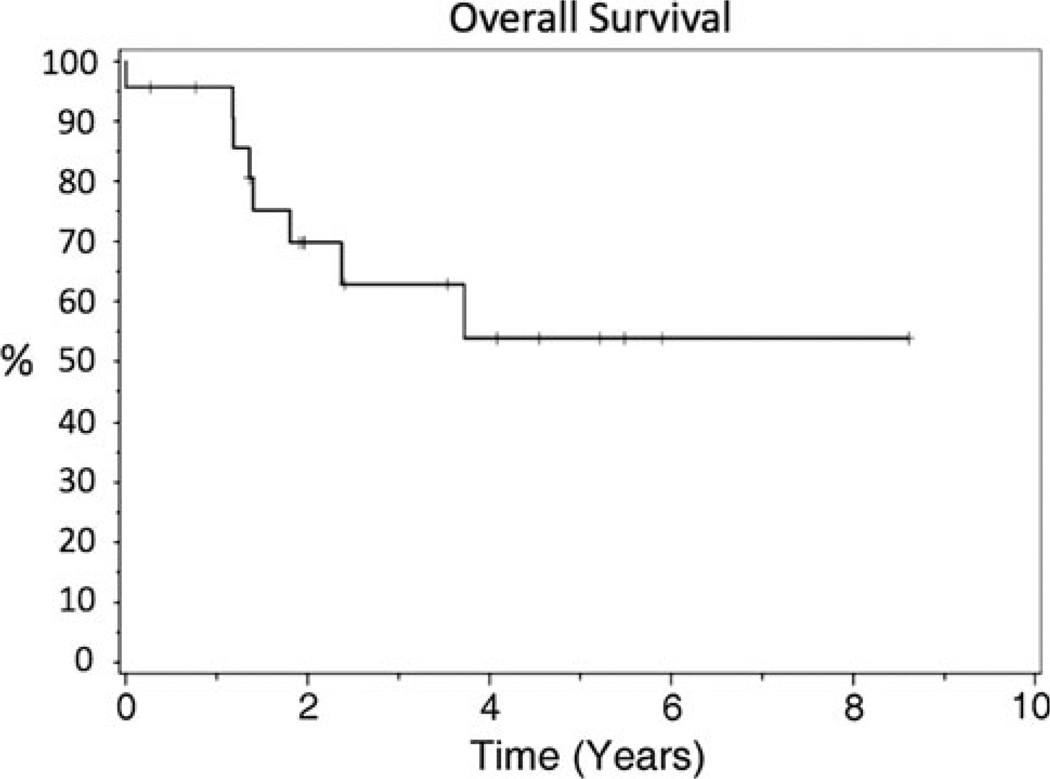
Atypical meningiomas have poor local control with emerging literature indicating the use of radiosurgery in treatment. The purpose of this study was to evaluate clinical outcomes including local control and failure pattern after Gamma Knife radiosurgery (GKRS) and factors that may affect these outcomes. Between 1999 and 2008, 24 patients were treated with GKRS as either primary or salvage treatment for pathologically proven atypical meningiomas. Treatment failures were determined by serial magnetic resonance imaging. A median marginal dose of 14 Gy was used (range 10.5-18 Gy). Overall local control rates at 1, 2, and 5 years were 75, 51, and 44%, respectively. With median follow-up time of 42.5 months, 14 of 24 patients experienced a treatment failure at time of last follow-up. Eight recurrences were in-field, four were marginal failures, and two were distant failures. Wilcoxon analysis revealed that the conformality index (CI) was a significant predictor of local recurrence (P = 0.04). CI did not predict for distant recurrences (P = 0.16). On multivariate analysis evaluating factors predicting progression free survival, dose >14 Gy was found to be statistically significant (P = 0.01). There appears to be a dose response using GKRS beyond 14 Gy but given the suboptimal local control rates in this study, higher doses may still be needed to obtain better local control.
Conflict of interest statement
Figures
References
-
- Whittle IR, Smith C, Navoo P, Collie D. Meningiomas. Lancet. 2004;363:1535–1543. - PubMed
-
- Jaaskelainen J. Seemingly complete removal of histologically benign intracranial meningioma: late recurrence rate and factors predicting recurrence in 657 patients. A multivariate analysis. Surg Neurol. 1986;26:461–469. - PubMed
-
- Harris AE, Lee JY, Omalu B, Flickinger JC, Kondziolka D, Lunsford LD. The effect of radiosurgery during management of aggressive meningiomas. Surg Neurol. 2003;60:298–305. (discussion 305) - PubMed
-
- Goyal LK, Suh JH, Mohan DS, Prayson RA, Lee J, Barnett GH. Local control and overall survival in atypical meningioma: a retrospective study. Int J Radiat Oncol Biol Phys. 2000;46:57–61. - PubMed
-
- Hug EB, Devries A, Thornton AF, et al. Management of atypical and malignant meningiomas: role of high-dose, 3D-conformal radiation therapy. J Neurooncol. 2000;48:151–160. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
